




-
桡动脉穿刺置管是麻醉科最常用的临床操作之一,实时动脉测压技术在危重、复杂、长时间手术中广泛应用。肥胖病人往往合并有高血压、糖尿病,术中血流动力学波动较大,动脉穿刺测压能大大提高围手术期安全性。传统的穿刺技术是靠操作者的手感,穿刺成功率不能保证,临床上经常遇到穿刺困难,有时候因为动脉穿刺困难延误时间达1 h甚至更长。超声在临床应用越来越普及,几乎所有的三级医院麻醉科均配备超声仪器,超声引导进行神经阻滞、动静脉穿刺、容量评估及肺超声、食管超声等,让围手术期的管理越来越精准。对于超声引导下动静脉穿刺技术,有报道[1]短轴平面外优于长轴平面内,也有报道[2]2种方法成功率类似,长轴平面内并发症更少。随着近年来高频超声的广泛应用,浅表超声技术大大提高了超声的清晰度,超声实时引导穿刺技术是一种趋势。根据本研究团队近年来大量进行超声引导下神经阻滞操作的经验,平面内操作通常优于平面外操作,尤其在安全性上。本研究通过随机对照研究比较超声引导下桡动脉长轴平面内穿刺和短轴平面外穿刺技术的优缺点,希望总结经验指导临床。现作报道。
HTML
-
本研究通过安徽医科大学第二附属医院医学伦理委员会批准,收集2019年6月至2020年5月需要进行动脉测压成年肥胖病人[体质量指数(BMI)≥28 kg/m2]100例,ASA Ⅰ~Ⅲ级,排除Allen试验阳性,尺动脉闭塞、外周血管疾病病人。随机分为超声引导短轴(S)组和超声引导长轴(L)组,2组病人年龄、性别比例、BMI、手术类别一般资料差异均无统计学意义(P>0.05)(见表 1),具有可比性。
分组 年龄/岁 男 女 BMI/(kg/m2) 手术类型 减重手术 非减重手术 S组 35±10 28 22 41.3±6.2 37 13 L组 37±13 31 19 42.0±7.7 41 9 t 0.86 0.37 0.50 0.93 P >0.05 >0.05 >0.05 >0.05 *示χ2值 -
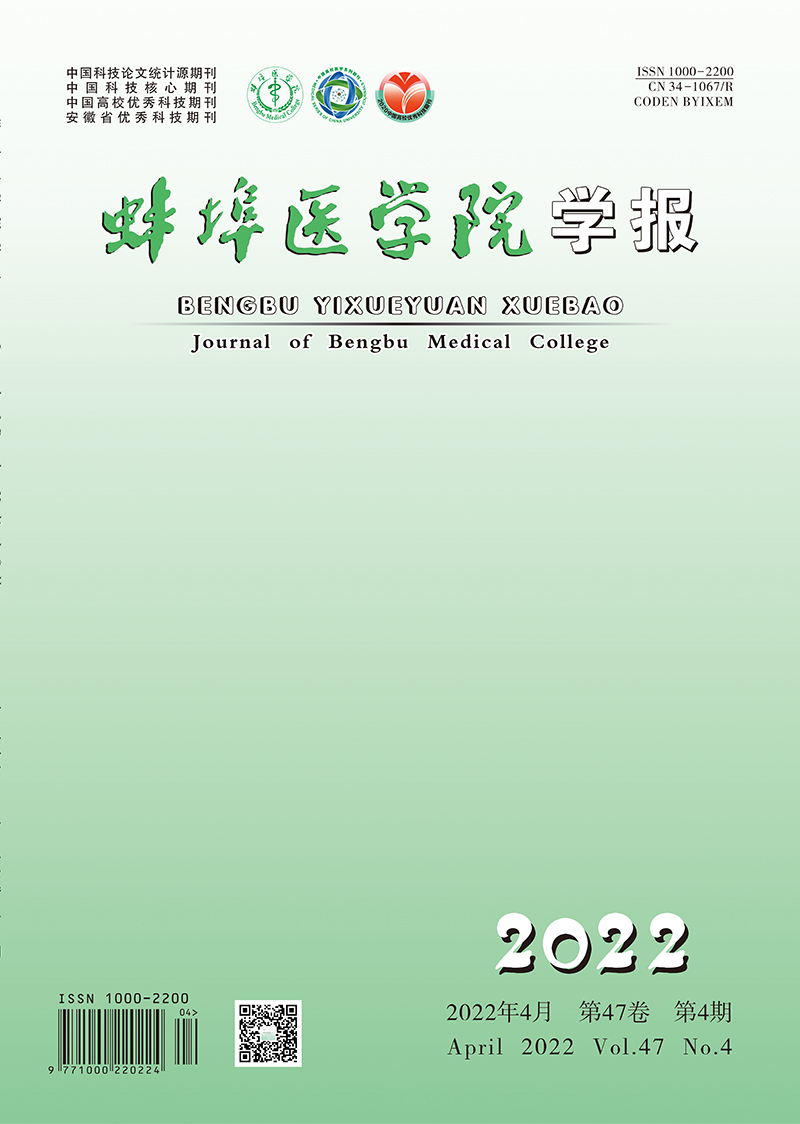
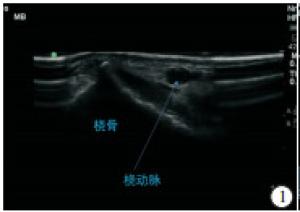
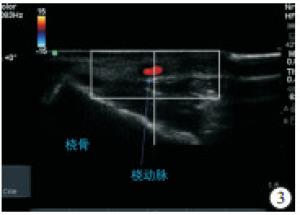
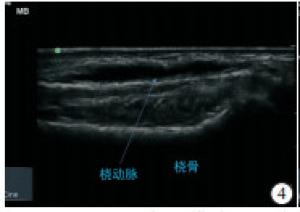
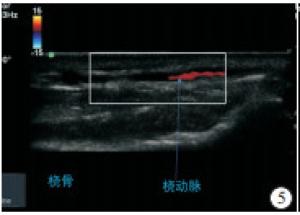
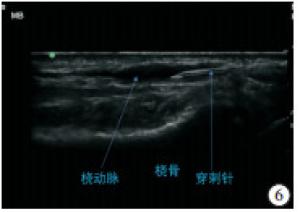
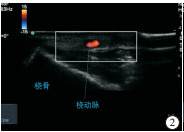
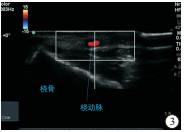
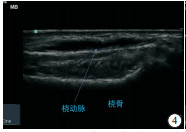
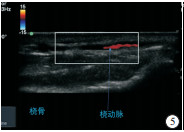
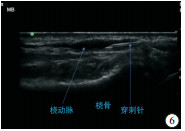
所有病人进入手术室首先进行信息核查确认,监护氧饱和度、心率、血压。心理关怀病人,告知操作事项,对于紧张病人静脉推注舒芬太尼5 μg,咪达唑仑1 mg。病人平卧位,穿刺侧上肢外展置于支架上,手腕处垫薄枕,固定手掌使腕部屈曲,掌心向上。超声探头(美国索诺声Edge Ⅱ,探头为6~13 MHz线阵探头)表面均有涂抹适量耦合剂,无菌透明贴膜包住超声探头,确保无菌操作。2D模式超声扫查桡动脉和尺动脉未见明显狭窄后继续操作;超声引导下S组:将探头放置桡骨茎突近端2~3 cm扫查到桡动脉,根据动脉的波动性识别桡动脉(见图 1),然后利用Color模式进行确定(见图 2),选择最清晰处穿刺,利用M模式确定中点,将M线对准动脉最宽处(见图 3),将探头的左右方向与超声显示屏左右一致,进针点离开探头0.5 cm 30°左右平面外进针,穿刺过程中可以在2D、M及Color不同模式之间切换,尽量使穿刺针在显示屏中间。超声引导下L组:利用相同方法确定动脉短轴中点后,缓慢旋转探头90°,保持动脉在视野中,通过轻微向桡侧或尺侧平移探头获取最宽的动脉图像后固定探头(见图 4、5),进针点离开探头0.5 cm 0°~30°平面内进针,全程确保针尖和针体可见(见图 6)。

-
比较2组穿刺一次成功率、穿刺时间(自穿刺点消毒至穿刺套管针置入完成), 使用穿刺针数量、穿刺次数(进针到皮肤至退针出皮肤定义为穿刺一次)以及穿刺部位血肿发生情况。
-
采用t检验、χ2检验和秩和检验。
1.1. 一般资料
1.2. 方法
1.3. 观测指标
1.4. 统计学方法
-
L组穿刺一次成功率高于S组(P < 0.05);S组4例出现穿刺部位血肿,均更换对侧桡动脉穿刺成功,L组未发生穿刺部位血肿,2组差异有统计学意义(P < 0.05);2组病人穿刺时间、穿刺次数、穿刺针使用数量差异均无统计学意义(P>0.05)(见表 2)。2组穿刺时间变异系数,S组为37.5 %,L组为16.7%。
分组 n 穿刺一次成功 穿刺时间/s 穿刺次数
M50(M25, M75)穿刺针数量
M50(M25, M75)/根穿刺部位血肿 S组 50 27(54.00) 48.3±18.1 1(1, 4) 1(1, 3) 4(8.00) L组 50 39(78.00) 52.4±9.0 1(1, 3) 1(1, 3) 0(0.00) t — 6.42* 1.43 — — 4.16* P — < 0.05 >0.05 >0.05 >0.05 < 0.05 *示χ2值
-
超声引导下的穿刺技术大大提高了麻醉医生穿刺成功率[3-6]。因为静脉穿刺的风险较大,超声引导下的静脉穿刺应用较为广泛,超声引导下动脉穿刺在临床应用并不十分广泛,但是临床上动脉穿刺困难发生率并不比静脉穿刺少[7-8]。因为外周动脉直径较小,在超声下并没有显示中心静脉那么容易,临床操作上需要一些技巧和经验,尤其肥胖病人,因为皮下脂肪较厚,穿刺困难常有发生。
本研究表明,L组穿刺一次成功率高于S组;S组4例出现穿刺部位血肿,均更换对侧桡动脉穿刺成功,L组未发生穿刺部位血肿,2组差异有统计学意义。不难理解,超声引导穿刺技术最明显的优势是可视化,让临床操作更精准,而平面内技术可以全程可视下操作,因此成功率高,并发症少。超声引导短轴平面外操作不能够全程可视,只能看到针尖或者针体的一部分,如果将针体当做针尖可能出现穿刺针偏离目标而没有发现。这些临床体会在做超声引导下神经阻滞时很容易获得,通常平面内穿刺技术是穿刺成功率和安全性最高的方法。超声引导长轴平面内可以全程可见穿刺针和穿刺目标动脉,因此穿刺成功率很高,并发症很少[9-10], 本研究中亦得到证实。
通常情况下,超声引导下桡动脉穿刺短轴平面外穿刺路径较短,长轴平面内穿刺路径较长;短轴法容易找到动脉,长轴法容易丢掉目标血管;因此通常认为超声引导下长轴穿刺需要更长的穿刺时间。本研究结果表明,2种方法穿刺平均时间差异无统计学意义。虽然超声引导下短轴平面外穿刺容易确定动脉,但是发生穿刺到动脉而置管不顺利的情况明显多于超声引导长轴平面内,短轴法穿刺时间变异系数较大,长轴法穿刺时间变异系数小;因此如果2组都穿刺顺利,都是一次穿刺成功,短轴法节约时间,当穿刺病例较多时,平均以后2组比较穿刺时间差异无统计学意义。因此,对于穿刺难度较大以及短轴穿刺失败的情况,选择超声引导长轴平面内穿刺技术会增加穿刺成功率[9]。
此外,超声引导下平面内桡动脉穿刺安全性高,穿刺并发症少,穿破桡动脉后壁造成血肿情况少。长轴平面内桡动脉穿刺技术真正发挥了超声实时引导,全程引导的优点,因此并发症少[10],当然长轴也有穿刺的缺点,例如容易在超声图像上丢失血管,临床实际操作过程中需要2种扫查方法结合。
 DownLoad:
DownLoad: