


-
结直肠癌是世界范围内常见的消化道恶性肿瘤,其发病率位于男性肿瘤的第三位,女性肿瘤的第二位。近年来随着诊治技术迅速发展,其5年生存率已经得到了很大提高[1-2]。但由于肿瘤的复发及化疗等原因,其临床疗效尚不能令人满意。因此,临床上仍然迫切需要寻求临床和生物标记物来提高结直肠癌病人的诊治效果。预后营养指数(prognostic nutritional index,PNI)是使用血清白蛋白和淋巴细胞的绝对值计算而来,最初用于评价外科病人的营养状态。近年来有研究表明PNI与肿瘤的发生发展有着密切的关系[3-4]。体质量指数(body mass index,BMI)是评价肥胖的可靠指标。最近国外有研究[5]表明BMI与食管癌的预后有关。然而目前国内外尚无研究使用PNI和BMI建立联合预测模型来评估结直肠癌病人术后预后。因此,该研究探讨PNI和BMI与病人预后关系,并评估二者的联合预测价值是否优于单独预测价值。现作报道。
-
选取2011年1月至2012年2月在我院术前病理诊断为结直肠癌且接受结直肠癌根治术的病人116例。所有病人资料齐全,术前均未接受放化疗,术前7 d常规完成胸片、腹盆腔CT、肠镜等常规检查。其中男60例,女56例;年龄19~85岁,其中>60岁62例,≤60岁54例;病理学组织学分型:高分化29例,中低分化87例。肿瘤分期参照美国癌症联合委员会(AJCC)TNM分期手册第7版[6]。116例病人中位随访时间为40.0个月(6~72个月)。本研究通过了我院伦理委员会的批准,纳入受试者及其监护人均签署知情同意书。
-
分析包括年龄、性别、肿瘤位置、肿瘤浸润深度、淋巴结转移数目、远处转移、临床分期等病人基本资料,同时调查分析病人入院后的PNI及BMI。术前营养状况评估所需血细胞计数及生化资料均来自于术前一周的常规实验室检查。PNI=血清白蛋白(g/L)+5×淋巴细胞绝对值(×109)。BMI定义为体质量/kg除以身高的平方/m2。WHO将BMI≤18.5 kg/m2认定为体质量过轻,因此,本研究将BMI分为2组:>18.5 kg/m2组(高BMI组)和≤18.5 kg/m2组(低BMI组)。根据病人术后5年生存结局指标绘制用PNI行预后评估的受试者工作特征曲线(ROC)曲线,选取约登指数最大时的PNI值为截断值。根据上述计算的截断值将本组病人分为高PNI组(术前PNI值>截断值)和低PNI组(术前PNI值≤截断值)。为了分析PNI和BMI的联合预测价值,我们将116例结直肠癌病人分为4组:A组为高PNI和高BMI组19例,B组为高PNI组和低BMI组28例, C组为低PNI和高BMI组34例,D组为低PNI和低BMI组35例。
-
采用χ2检验或Fisher′s确切概率法,采用生存分析(Kaplan-Meier法和Cox多因素回归模型)及log-rank检验生存曲线间的差异。
-
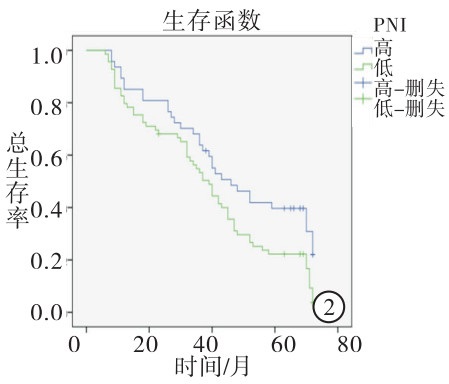
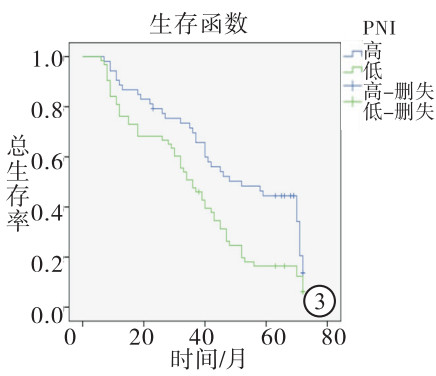
根据病人术后5年生存结局使用ROC曲线选取敏感性和特异性均较高的PNI值为截断值,PNI的截断值为47.5(约登指数为1.133)(见图 1)。47例高PNI组5年生存率40.4%高于69例低PNI组的5年生存率21.7%(χ2=4.712,P<0.05)(见图 2)。BMI>18.5 kg/m2病人53例,5年生存率43.4%,BMI≤18.5 kg/m2病人63例,5年生存率15.9%。高BMI组5年生存率高于比低BMI组的5年生存率(χ2=10.71,P<0.01)(见图 3)。
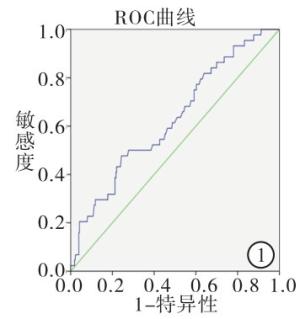
图 1 工作特征曲线取PNI截断值ROC曲线
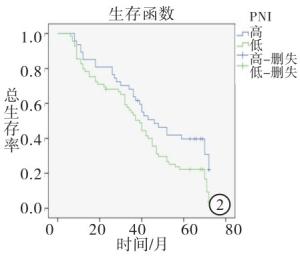
图 2 PNI与结直肠癌病人术后5年总生存率关系
图 3 BMI与结直肠癌病人术后5年总生存率关系
-
Kaplan-Meier法分析结果提示,PNI和BMI影响结直肠癌预后。高PNI组中位生存时间为46.00个月(95% CI:32.94~59.06),大于低PNI组中位生存时间39.00个月(95% CI:32.99~45.01)(χ2=5.72,P<0.05)(见图 2)。高BMI组中位生存时间为52.00个月(95% CI:32.09~71.09.00),高于低BMI组平均生存时间36.00 d(95% CI:29.26~49.74)(χ2=8.01,P<0.01)(见图 3)。将病人性别、年龄、肿瘤位置、肿瘤分化程度、浸润深度、淋巴结转移、远处转移、临床分期、PNI和BMI进行单因素多重变量的Cox等比例风险模型分析,结果表明肿瘤分化、浸润深度、淋巴结转移、远处转移、临床分期、PNI和BMI对病人预后有意义(P<0.05~P<0.01)。将单因素分析有意义的变量纳入多因素分析,结果表明肿瘤分化、远处转移、临床分期、PNI、BMI等与病人预后有关系(P<0.05),其中低PNI病人死亡风险是高PNI病人死亡风险的1.752倍(95%CI:1.131~2.713)(P<0.05),低BMI病人死亡风险是高病人死亡风险的1.620倍(95%CI:1.052~2.495)(P<0.05)(见表 1)。
自变量 单因素分析结果 多因素分析结果 HR 95% CI χ2 P HR 95% CI χ2 P 年龄 1.144 0.762~1.716 0.42 >0.05 — — — — 性别 1.192 0.796~1.783 0.73 >0.05 — — — — 肿瘤位置 1.231 0.946~1.601 2.41 >0.05 — — — — 分化程度 0.428 0.259~0.705 12.72 <0.01 0.575 0.335~0.989 3.99 <0.05 浸润深度 1.343 1.086~1.661 7.76 <0.01 — — — — 淋巴结转移 1.280 1.001~1.635 3.36 <0.05 — — — — 远处转移 57.166 5.184~630.661 5.71 <0.01 21.015 1.827~241.723 5.97 <0.05 临床分期 1.605 1.243~2.072 13.55 <0.01 1.349 1.025~1.776 4.55 <0.05 脉管侵犯 0.750 0.467~1.206 1.34 >0.05 — — — — 神经侵犯 0.629 0.370~1.070 2.66 >0.05 — — — — PNI 1.648 1.075~2.526 5.49 <0.05 1.752 1.131~2.713 6.32 <0.05 BMI 1.774 1.173~2.684 7.56 <0.01 1.620 1.052~2.495 4.79 <0.05 表 1 结直肠癌病人单因素和多因素生存分析
-
PNI和BMI联合预测价值D组与第A、B、C组比较,均具有较低的1、3、5年生存率(P<0.01)(见表 2)。低PNI且低BMI病人预示着更差的预后,因此PNI和BMI联合预测结直肠癌预后相较于单独作用更加精确(见图 4)。
分组 n 1年生存 3年生存 5年生存 A组 19 19(100.0) 14(73.7) 9 (47.4) B组 28 27(96.4) 18(64.3) 8(28.3) C组 34 34(100.0) 23(67.6) 13(38.2) D组 35 28(80.0)** △△## 15(42.9)**△△## 0(0.0)**△△## 合计 116 109(94.0) 70(60.3) 30(25.9) χ2 — 13.37 6.83 19.62 P — 0.003 0.078 <0.01 χ2分割检验:与A组比较**P<0.01;与B组比较△△P<0.01;与C组比较##P<0.01 表 2 4组病人生存情况的比较[n; 百分率(%)]
图 4 PNI与BMI联合判断病人术后5年总体生存率
-
PNI和BMI数值仅需通过住院病人的常规血液检查或简单测量即可得到,经济方便,不增加病人负担,是临床常用的免疫营养状况评价指标。同时结直癌预后与代谢、内分泌、免疫、营养等多方面因素密切相关。因此PNI和BMI作为免疫营养状态的评价指数,可能与结直肠癌预后相关[7-8]。本研究探讨了PNI和BMI在结直肠癌病人术后预后中的评估价值,结果显示术前PNI、BMI与病人术后预后相关,提示二者在预测结直肠癌病人术后预后方面具有一定的临床价值。
PNI作为免疫营养状况的有效判断指标,由血清白蛋白和淋巴细胞的绝对值计算而来,最初由日本学者建立,用来评估外科营养状况、预测手术风险及并发症发生率。近年来有研究表明PNI与炎症、多种肿瘤预后相关,尤其是胰腺炎、消化道肿瘤如胃癌、肝癌、结直肠癌等[9-15]。当白蛋白<25 g/L时,提示急性胰腺炎病人预后较差。淋巴细胞绝对值的降低与许多疾病严重程度有关,甚至是一些疾病的独立预后因素。白蛋白的降低或淋巴细胞绝对值的减少,预示着许多疾病预后不良。CAO等[15]研究表明,PNI<44.55时,结直肠癌病人术后发生感染、吻合口瘘等并发症机率增加,同时预示着5年生存率较低。本研究表明高PNI病人较低PNI病人远期生存率更高,与国内外研究结果相一致。但低PNI结直肠癌病人预后较差的机制目前仍不十分清楚,可能是营养不良与病人免疫抑制相关[16-17]。同时淋巴细胞是机体免疫系统的重要组份,在机体抵抗肿瘤过程中发挥着重要作用, 淋巴细胞绝对值的减少意味着抗肿瘤能力降低[18]。
BMI是另一个能够判断病人免疫营养状况的有效指标,低BMI(≤18.5 kg/m2)常预示着免疫抑制。既往研究表明与胃肠道肿瘤术后并发症发生风险,但近年来越来越多的证据表明BMI与肿瘤预后相关[7, 19-23]。FERGUSON等[21]一项纳入1 369例肺癌病人的回顾性研究表明,低BMI肺癌病人具有更高的并发症发生率和死亡率。同时,有研究表明食管癌病人中高BMI高的病人术后并发症较多,但生存期明显延长[7]。SMITH等[22-23]研究表明,BMI与食管癌分期和分化有关。目前BMI与结直肠癌的预后关系国内外研究较少。本研究生存分析结果表明高BMI组比低BMI组5年生存率更高,提示BMI可能与结直肠癌病人预后存在相关性。
虽然越来越多证据表明,PNI和BMI与肿瘤病人预后相关,但其预测的准确性仍存在争议。SONG等研究表明PNI能够预测病人预后,但相对NLR预测准确性较差[24]。ITOH等[25-26]对BMI预测肝癌预后的准确性也存在异议[25-26]。EJAZ等[27]使用血清白蛋白水平联合BMI预测模型提高了BMI预测胃癌预后的准确性。结果表明,本研究中低PNI且低BMI组病人较其他各组相比预后更差,差异有统计学意义。PNI和BMI联合评估结直肠癌病人的预后,增加了判断的准确率。
综上所述,PNI、BMI与结直肠癌病人预后存在相关性并且经济方便,可能成为预测结直肠癌病人预后的临床标志物,适宜在临床上广泛推广。同时,PNI和BMI联合评估预后能够提高准确性,有望将联合评估模型用于评估病人预后,从而在术前制定相应的营养及辅助治疗策略。同时,本研究样也存在一定局限性。研究样本量较小,研究模型仍需更大规模的临床研究验证;PNI在现有研究中的截断值各有不同,仍需大样本的研究来探索统一的标准;PNI与BMI预测病人预后的机制尚需进一步的研究。
术前营养预后指数和体质量指数与结直肠癌病人预后关系的研究
Study on the correlations of the PNI and BMI with prognosis in patients with colorectal cancer
-
摘要:
目的探讨术前营养预后指数(PNI)和体质量指数(BMI)与结直肠癌病人术后预后的关系。 方法选取接受结直肠癌根治术的病人116例,使用受试者工作特征曲线曲线得出PNI的截断值。使用Kaplan-Meier法绘制术后生存曲线,Cox回归模型分析影响术后生存的独立影响因素。 结果PNI的截断值为47.5,高PNI组5年生存率36.2%高于低PNI组的18.8%(P < 0.05);单因素分析表明肿瘤分化程度、浸润深度、淋巴结转移、远处转移、临床分期、PNI、BMI与病人预后相关(P < 0.05~P < 0.01)。Cox多因素分析结果表明分化程度、远处转移、临床分期、PNI和BMI是结直肠癌根治术后病人预后的独立影响因素(P < 0.05)。PNI与BMI联合预测病人预后价值高于其单独预测价值。 结论PNI与BMI是结直肠癌病人术后预后的独立影响因素,使用PNI与BMI联合评估病人预后能够提高准确性。 Abstract:ObjectiveTo explore the correlations of the prognostic nutritional index(PNI) and body mass index(BMI) with prognosis in patients with colorectal cancer. MethodsThe clinicopathological data of 116 colorectal cancer patients treated with radical colectomy were retrospectively analyzed.The receiver operating characteristic curve was used to determine the cut-off value of PNI, the survival curve was plotted using the Kaplan-Meier method, and the cox regression model was used to analyze the independent factor affecting postoperative. ResultsThe cut-off value of PNI was 47.5.The 5-year survival rate in high P survival NI group(36.2%) was higher than that in low PNI group(18.8%)(P < 0.05).The results of univariate analysis showed that the tumor differentiation, invasion depth, lymph node metastasis, distant metastasis, clinical staging, PNI and BMI were correlation with prognosis of patients(P < 0.05 to P < 0.01).The results of Cox multi-factor analysis showed that the tumor differentiation, distant metastasis, clinical staging, PNI and BMI were the independent factor affecting prognosis of patients(P < 0.05).The value of PNI combined with BMI in predicting the prognosis of patients was higher than that of PNI or BMI(P < 0.05). ConclusionsPNI and BMI are the independent factors affecting prognosis of patients with colorectal cancer, and the combination of PNI with BMI can improve the accuracy in evaluating prognosis of patients. -
Key words:
- colorectal cancer /
- prognostic nutritional index /
- body mass index
-
表 1 结直肠癌病人单因素和多因素生存分析
自变量 单因素分析结果 多因素分析结果 HR 95% CI χ2 P HR 95% CI χ2 P 年龄 1.144 0.762~1.716 0.42 >0.05 — — — — 性别 1.192 0.796~1.783 0.73 >0.05 — — — — 肿瘤位置 1.231 0.946~1.601 2.41 >0.05 — — — — 分化程度 0.428 0.259~0.705 12.72 <0.01 0.575 0.335~0.989 3.99 <0.05 浸润深度 1.343 1.086~1.661 7.76 <0.01 — — — — 淋巴结转移 1.280 1.001~1.635 3.36 <0.05 — — — — 远处转移 57.166 5.184~630.661 5.71 <0.01 21.015 1.827~241.723 5.97 <0.05 临床分期 1.605 1.243~2.072 13.55 <0.01 1.349 1.025~1.776 4.55 <0.05 脉管侵犯 0.750 0.467~1.206 1.34 >0.05 — — — — 神经侵犯 0.629 0.370~1.070 2.66 >0.05 — — — — PNI 1.648 1.075~2.526 5.49 <0.05 1.752 1.131~2.713 6.32 <0.05 BMI 1.774 1.173~2.684 7.56 <0.01 1.620 1.052~2.495 4.79 <0.05  下载: 导出CSV
下载: 导出CSV
表 2 4组病人生存情况的比较[n; 百分率(%)]
分组 n 1年生存 3年生存 5年生存 A组 19 19(100.0) 14(73.7) 9 (47.4) B组 28 27(96.4) 18(64.3) 8(28.3) C组 34 34(100.0) 23(67.6) 13(38.2) D组 35 28(80.0)** △△## 15(42.9)**△△## 0(0.0)**△△## 合计 116 109(94.0) 70(60.3) 30(25.9) χ2 — 13.37 6.83 19.62 P — 0.003 0.078 <0.01 χ2分割检验:与A组比较**P<0.01;与B组比较△△P<0.01;与C组比较##P<0.01
下载: 导出CSV
-
[1] NISHIHARA R, OGINO S, CHAN AT.Colorectal-cancer incidence and mortality after screening[J].N Engl J Med, 2013, 369(24):2355. [2] SIEGEL R, DESANTIS C, VIRGO K, et al.Cancer treatment and survivorship statistics, 2012[J].CA Cancer J Clin, 2012, 62(4):220. doi: 10.3322/caac.v62:4 [3] KANG MY, CHUANG CT, SUNG HH, et al.Prognostic Significance of Pre-to Postoperative Dynamics of the Prognostic Nutritional Index for Patients with Renal Cell Carcinoma Who Underwent Radical Nephrectomy[J].Ann Surg Oncol, 2017, 24(13):4067. doi: 10.1245/s10434-017-6065-2 [4] 宋国栋, 王力, 沈洪, 等.预后营养指数在老年胃癌病人治疗与预后中的意义[J].中华普通外科杂志, 2017, 32(4):293. doi: 10.3760/cma.j.issn.1007-631X.2017.04.003 [5] TMIYAZAKI, SAKAI M, SOHDA M, et al.Prognostic Significance of Inflammatory and Nutritional Parameters in Patients with Esophageal Cancer[J].Anticancer Res, 2016, 36(12):6557. doi: 10.21873/anticanres [6] EDGE SB, BYRD DR, COMPTON CC, et al.The American Joint Committee on Cancer:the 7th edition of the AJCC cancer staging manual and the future of TNM[J].Ann Surg Oncol, 2010, 17(6):1471. doi: 10.1245/s10434-010-0985-4 [7] MCMILLAN DC.Systemic inflammation, nutritional status and survival in patients with cancer[J].Curr Opin Clin Nutr Metab Care, 2009, 12(3):223. doi: 10.1097/MCO.0b013e32832a7902 [8] SERETIS C, KAISARI P, WANIGASOORIYA K, et al.Malnutrition is associated with adverse postoperative outcome in patients undergoing elective colorectal cancer resections[J].J BUON, 2018, 23(1):36. [9] GONZALVEZ-GASCH A, DE CASASOLA GG, MARTIN RB, et al.A simple prognostic score for risk assessment in patients with acute pancreatitis[J].Eur J Intern Med, 2009, 20(3):e43. doi: 10.1016/j.ejim.2008.09.014 [10] DE JAGER CP, VAN WIJK PT, MATHOERA RB, et al.Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit[J].Crit Care, 2010, 14(5):R192. doi: 10.1186/cc9309 [11] LE TULZO Y, PANGAULT C, GACOUIN A, et al.Early circulating lymphocyte apoptosis in human septic shock is associated with poor outcome[J].Shock, 2002, 18(6):487. doi: 10.1097/00024382-200212000-00001 [12] PEZZILLI R, BILLI P, BELTRANDI E, et al.Circulating lymphocyte subsets in human acute pancreatitis[J].Pancreas, 1995, 11(1):95. doi: 10.1097/00006676-199507000-00010 [13] JI F, LIANG Y, FU S, et al.Prognostic value of combined preoperative prognostic nutritional index and body mass index in HCC after hepatectomy[J].HPB, 2017, 19(8):695. doi: 10.1016/j.hpb.2017.04.008 [14] JIANG N, DENG JY, LIU Y, et al.The role of preoperative neutrophil-lymphocyte and platelet-lymphocyte ratio in patients after radical resection for gastric cancer[J].Biomarkers, 2014, 19(6):444. doi: 10.3109/1354750X.2014.926567 [15] CAO X, ZHAO G, YU T, et al.preoperative prognostic nutritional index correlates with severe complications and poor survival in patients with colorectal cancer undergoing curative laparoscopic surgery:a retrospective study in a single chinese institution[J].Nutr Cancer, 2017, 69(3):454. doi: 10.1080/01635581.2017.1285038 [16] GUPTA D, LIS CG.Pretreatment serum albumin as a predictor of cancer survival:a systematic review of the epidemiological literature[J].Natr, 2010, 22(9):69. [17] LI G, GAO J, LIU ZG, et al.Influence of pretreatment ideal body weight percentile and albumin on prognosis of nasopharyngeal carcinoma:long-term outcomes of 512 patients from a single institution[J].Head Neck, 2014, 36(5):660. doi: 10.1002/hed.v36.5 [18] ROSENBERG SA.Progress in human tumour immunology and immunotherapy[J].Nature, 2001, 411(6835):380 doi: 10.1038/35077246 [19] 谭卫民, 莫隽全, 邓伟雄, 等.老年结直肠癌术后肺部并发症危险因素分析[J].中国普通外科杂志, 2006, 15(2):150. doi: 10.3969/j.issn.1005-6947.2006.02.019 [20] 韩加刚, 王振军, 魏广辉, 等.择期结直肠癌一期吻合术后切口感染预后因素的回顾性队列研究[J].中华外科杂志, 2014, 52(6):415. doi: 10.3760/cma.j.issn.0529-5815.2014.06.004 [21] FERGUSON MK, IM HK, WATSON S, et al.Association of body mass index and outcomes after major lung resection[J].Eur J Cardiothorac Surg, 2014, 45(4):e94. doi: 10.1093/ejcts/ezu008 [22] SMITH M, ZHOU M, WHITLOCK G, et al.Esophageal cancer and body mass index:results from a prospective study of 220, 000 men in China and a meta-analysis of publishedstudies[J].Int J Cancer 2008, 122(7):1604. [23] SUN P, ZHANG F, CHEN C, et al.Comparison of the prognostic values of various nutritional parameters in patients with esophageal squamous cell carcinoma from Southern China[J].J Thorac Dis, 2013, 5(4):484. [24] SONG Y, YANG Y, GAO P, et al.The preoperative neutrophil to lymphocyte ratio is a superior indicator of prognosis compared with other inflammatory biomarkers in resectable colorectal cancer[J].BMC Cancer, 2017, 17(1):744. doi: 10.1186/s12885-017-3752-0 [25] ITOH S, SHIRABE K, MATSUMOTO Y, et al.Effect of body composition on outcomes after hepatic resection for hepatocellular carcinoma[J].Ann Surg Oncol, 2014, 21(9):3063. doi: 10.1245/s10434-014-3686-6 [26] SCHUTTE K, TIPPELT B, SCHULZ C, et al.Malnutrition is a prognostic factor in patients with hepatocellular carcinoma (HCC)[J].Clin Nutr, 2015, 34(6):1122. doi: 10.1016/j.clnu.2014.11.007 [27] EJAZ A, SPOLVERATO G, KIM Y, et al.Impact of body mass index on perioperative outcomes and survival after resection for gastric cancer[J].J Surg Res, 2015, 195(1):74. doi: 10.1016/j.jss.2014.12.048 -

 点击查看大图
点击查看大图
图(4)表(2)
计量
- 文章访问数: 32133
- HTML全文浏览量: 14835
- PDF下载量: 57
- 被引次数: 0
