

-
目前,由于在我国女性盆底功能障碍(PFD)不受重视以及缺乏有效的早期诊断方法,就诊时多数病人已经出现比较严重的临床症状,如果能够在早期对该疾病进行诊断,多数病人可避免手术治疗,通过盆底肌肉功能训练等达到治疗的目的[1]。盆底超声是近年开始应用于临床的一种无创、简便的评估盆底功能的影像学方法,本研究采用经会阴实时三维盆底超声观察不同分娩方式在静息状态下、最大Valsalva动作后对产后女性肛提肌裂孔面积的影响,以期为临床提供早期、有效的诊断及疗效评估的依据。现作报道。
-
选取2017年3-12月我院行盆底三维超声检查的产后6周初产妇80例(病例组)及行常规妇科超声检查的未生育育龄女性40例(对照组)。记录所有产后及未生育女性的年龄、身高、体质量、新生儿出生体质量及有无漏尿等临床症状资料;剔除不能配合完成有效的Valsalva动作者、泌尿系感染者、既往有盆腔手术史者及产钳使用者。对照组均有性生活史。病例组与对照组的年龄、体质量指数均具有可比性。按分娩方式将病例组分为经阴道分娩组51例和选择性剖宫产组29例。所有受检者均知情同意。
-
采用美国GE Volusion E8型彩色多普勒超声诊断仪,配置RAB4-8L容积探头,探头频率4.0~8.0 MHz,二维扫查角度为70°,实时三维容积角度为85°。
-
受检者检查前需排空膀胱和直肠,仰卧于检查床上,取截石位,选择经腹部三维容积探头,调节好仪器各项参数,外套灭菌专用探头套,紧贴两侧大阴唇之间放置,获得盆底标准正中矢状面,以耻骨联合后下缘为参考点,从前往后主要包括前盆腔的耻骨联合、尿道、膀胱颈;中盆腔的阴道、宫颈;后盆腔的直肠、直肠壶腹部、肛管。对受检者静息状态下和最大Valsalva动作后(即病人屏气并向下用力至最大腹压时)的图像分别进行采集和储存,采用三维重建成像软件进行后处理,在肛提肌裂孔标准平面[2]分别测量静息状态下和最大Valsalva动作后肛提肌裂孔面积。
-
采用方差分析、q检验和直线相关分析。
-
3组在静息状态下和最大Valsalva动作后肛提肌裂孔面积比较差异均有统计学意义(P < 0.01),选择性剖宫产组和对照组均低于经阴道分娩组(P < 0.05和P < 0.01),对照组均明显低于选择性剖宫产组(P < 0.01)(见表 1)。
分组 n 静息状态 最大Valsalva动作 经阴道分娩组 51 16.14±2.68 25.86±3.36 选择性剖宫产组 29 14.90±2.04* 23.14±2.17** 对照组 40 11.98±1.33**△△ 15.13±1.34**△△ F — 42.49 203.11 P — <0.01 <0.01 MS组内 — 4.655 6.570 q检验:与经阴道分娩组比较*P < 0.05,**P < 0.01;与选择性剖宫产组比较△△P < 0.01 表 1 3组不同状态下肛提肌裂孔面积比较(x±s;cm2)
-
分别将经阴道分娩组在静息状态、最大Valsalva动作后肛提肌裂孔面积与新生儿出生体质量进行相关性分析,二者均呈正相关关系(r=0.865、0.876)(见图 1)。
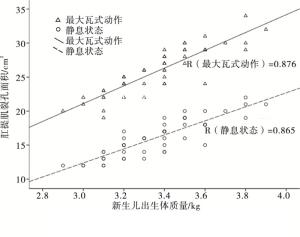
图 1 经阴道分娩组不同状态下肛提肌裂孔面积与新生儿出生体质量间相关性分析
-
女性盆底是一个复杂而紧密的支持系统,由封闭骨盆出口的多层肌肉、筋膜及韧带等构成。女性在未孕时,正常腹腔压力对子宫的影响力朝向骶骨和尾骨;腹腔压力增加时,腰部向前突出,腹部向前、向下突出,腹腔的压力将子宫向下向阴道的方向推,因此,女性在怀孕时,子宫是向下移位的,盆底肌肉会受到向下的压力而逐渐松弛。经阴道分娩过程中,盆底肌群整体延伸、扩张,肌肉、筋膜及神经会被牵拉损伤;胎儿及其附属物的长期压迫可能减少盆底支持结构的血液供应,使其发生缺血、缺氧,此外,产程时间的影响,特别是第二产程的延长及产钳使用情况等均对盆底支持结构产生不同程度的影响,可能导致女性PFD的发生[3]。MANT等[4]研究显示,在妊娠和产后发生PFD的相对危险系数是10.8。也有研究[5-6]发现阴道分娩,尤其是难产,会对肛提肌及盆内筋膜等盆腔支持组织造成不同程度的损伤,从而导致女性盆腔脏器脱垂(POP)及压力性尿失禁(SUI),且发生的概率随着分娩次数的增加而增加。
女性盆底支持结构在水平方向上可分为三个水平,第一水平由主韧带-骶韧带复合体组成;第二水平由肛提肌群及直肠阴道筋膜组成;第三水平由会阴体及括约肌组成。其中肛提肌群是盆底主要支撑结构,由髂骨尾骨肌、耻骨直肠肌与耻骨尾骨肌共同组成。妊娠、分娩或肛提肌损伤是导致盆底支持结构薄弱或损伤的主要原因,可导致盆底肌的顺应性、弹性降低,三块组成肌肉间形成的肛提肌裂孔在POP、SUI的发生、发展中扮演着重要的角色,肛提肌裂孔的大小可反映盆底支持结构及盆底肌的顺应性和弹性,肛提肌裂孔面积能够直接反映肛提肌裂孔的大小,是产后评估盆底损伤情况常用的指标。徐娆等[7]研究表明肛提肌裂孔面积与SUI间存在着一定的相关性。
目前,随着实时三维超声成像技术的发展,超声检查已经成为诊断产后女性PFD的首选影像学方法[8]。经会阴实时三维盆底超声能够获得盆底的轴平面,更加直观地显示盆底结构,利用TUI等模式进行多平面成像,采集动态图像并对数据进行后处理分析,可以动态、实时观察肛提肌裂孔的完整性及其形态的变化,其诊断价值与MRI相似,并且可以准确测量裂孔的面积,在观察细节方面经会阴实时三维盆底超声更具优势[9]。本研究采用实时三维盆底超声技术,对不同分娩方式产后女性的肛提肌裂孔面积进行研究,观察在静息状态下和最大Valsalva动作后两种状态下女性肛提肌裂孔面积的变化,并与对照组进行比较,分析不同分娩方式对女性肛提肌裂孔面积的影响,以推测盆底结构是否存在异常。由于在分娩后6周左右盆腔各器官位置已基本恢复至妊娠前状态,所以本研究选取产后6周复查女性,有利于评估分娩对盆底功能造成的近期影响。
本研究结果表明:在静息状态下及最大Valsalva动作后,病例组与对照组肛提肌裂孔面积比较差异有统计学意义,表明女性妊娠、分娩是导致PFD的重要原因之一,这与目前已有的研究[10]是接近的。在静息状态下,经阴道分娩组与选择性剖宫产组的盆底超声表现类似,肛提肌裂孔面积经比较差异无统计学意义,而2组最大Valsalva动作后的肛提肌裂孔面积显示出明显差异,提示不能单纯在静息状态下观察肛提肌裂孔的变化,必须结合最大Valsalva动作后的观察,得出的检查结果才具有诊断意义。在最大Valsalva动作后经阴道分娩组肛提肌裂孔面积明显大于选择性剖宫产组,说明经阴道分娩对肛提肌可能造成损伤,从而使得盆底支撑结构薄弱,可能是产后发生POP及SUI的高危因素。LIU等[11]研究表明经阴道分娩组SUI的发生率高于剖宫产组,与本研究结果一致。本研究发现,最大Valsalva动作后的肛提肌裂孔面积能更好地反映产后女性盆底支撑结构改变情况,可推荐作为产后女性常规筛查的评估指标。
本研究发现,经阴道分娩组在不同状态下肛提肌裂孔面积与新生儿出生体质量间均呈正相关关系,表明随着新生儿出生体质量的增加,肛提肌受损的概率随之增大,提示临产期胎儿体质量的估测对于阴道分娩过程中盆底支撑结构的保护具有非常重要的警示作用。
综上所述,经会阴实时三维盆底超声可通过测量不同状态下肛提肌裂孔面积来评估不同分娩方式对盆底功能的影响,最大Valsalva动作后的检测价值优于静息状态。
实时三维盆底超声评估不同分娩方式对产后女性肛提肌裂孔的影响
Effect of different delivery ways on postpartum hiatus of levator ani evaluated by real-time three-dimensional pelvic floor ultrasound
-
摘要:
目的采用经会阴实时三维盆底超声探讨不同分娩方式对产后女性肛提肌裂孔面积的影响。 方法选取就诊的80例产后6周女性(病例组)及40例未生育女性(对照组)作为研究对象,病例组又分为经阴道分娩组和选择性剖宫产组,对3组在静息状态下、最大Valsalva动作后肛提肌裂孔面积进行比较,评估不同分娩方式对产后女性肛提肌裂孔的影响,并将不同状态下经阴道分娩组肛提肌裂孔面积与新生儿出生体质量进行相关性分析。 结果3组在静息状态下和最大Valsalva动作后肛提肌裂孔面积比较差异有统计学意义(P < 0.01),选择性剖宫产组和对照组均低于经阴道分娩组(P < 0.05~P < 0.01),对照组低于选择性剖宫产组(P < 0.01);经阴道分娩组在静息状态下、最大Valsalva动作后肛提肌裂孔面积与新生儿出生体质量间均呈正相关关系(r=0.865、0.876)。 结论经会阴实时三维盆底超声可以通过测量肛提肌裂孔面积对产后女性盆底结构进行评估,具有无创简便、重复性好等优点,可以作为评估女性盆底功能的常规筛查方法,为临床诊断和治疗效果评价提供依据。 Abstract:ObjectiveTo investigate the effects of different delivery ways on the area of postpartum hiatus of levator ani evaluated by real-time three-dimensional pelvic floor ultrasound. MethodsEighty postpartum 6 weeks women and 40 nulliparous women were divided into the case group and control group, respectively.The case group was subdivided into the transvaginal delivery group and selective cesarean section group.The areas of postpartum hiatus of levator ani at rest and after the maxium Valsalva movement among three groups were compared, the effects of different delivery ways on the area of postpartum hiatus of levator ani were evaluated, and the correlation of the area of hiatus of levator ani in different states with neonatal weight was anlayzed in transvaginal delivery group. ResultsThe differences of the areas of hiatus of levator ani at rest and after the maxium Valsalva movement among three groups were statistically significant(P < 0.01), which in selective cesarean section group and control group was lower than that in transvaginal delivery group(P < 0.05 to P < 0.01), ans which in control group was lower than that in selective cesarean group(P < 0.01).The area of hiatus of levator ani at rest and after the maxium Valsalva movement in transvaginal delivery group was positively correlated with neonatal weight(r=0.865, 0.876). ConclusionsThe transperineal real-time three-dimensional ultrasound in evaluating the postpartum pelvic floor structure by measuring the area of hiatus of levator ani is noninvasive, convenient and repetitive, which can be used as a routine screening method, and provide the basis in the evaluation of clinic diagnosis and treatment effect. -
表 1 3组不同状态下肛提肌裂孔面积比较(x±s;cm2)
分组 n 静息状态 最大Valsalva动作 经阴道分娩组 51 16.14±2.68 25.86±3.36 选择性剖宫产组 29 14.90±2.04* 23.14±2.17** 对照组 40 11.98±1.33**△△ 15.13±1.34**△△ F — 42.49 203.11 P — <0.01 <0.01 MS组内 — 4.655 6.570 q检验:与经阴道分娩组比较*P < 0.05,**P < 0.01;与选择性剖宫产组比较△△P < 0.01  下载: 导出CSV
下载: 导出CSV
-
[1] 杨晓, 刘玉玲.盆底肌肉训练对产后盆底功能障碍的效果分析[J].国际妇产科学杂志, 2013, 40(2):164. [2] 张新玲, 黄泽萍, 毛永江.盆底超声的临床应用[M].广州:暨南大学出版社, 2013:33. [3] ORTVEIT G, BROWN JS, THORN DH, et al.Symptomatic pelvic organ prolapse:prevalence and risk factors in a population-based, racially diverse cohort[J].Obstet Gynecol, 2007, 109(6):1396. doi: 10.1097/01.AOG.0000263469.68106.90 [4] MANT J, PAINTER R, VESSEY M.Epidemiology of genital pmlapse:obser:vations from the oxford family planning association study[J].Br J Obstet Gynecol, 1997, 104(5):579. doi: 10.1111/bjo.1997.104.issue-5 [5] O'BOYLE AL, O'BOYLE JD, CALHOUN B, et al.Pelvic organ support in pregnancy and postpartum[J].Int Urogynecol J Pelvic Floor Dysfunct, 2005, 16(1):69. doi: 10.1007/s00192-004-1210-4 [6] AYDN S, TUNCEL MA, AYDN CA, et al.Do weprotectthepelvic floor with non-electivecesarean A study of 3-D/4-D pelvic floor ultrasound immediateIyafter delivery[J].J Obstet Gynaecol Res, 2014, 40(4):1037. doi: 10.1111/jog.2014.40.issue-4 [7] 徐娆, 史铁梅, 林琳, 等.超声评价女性压力性尿失禁病人盆膈裂孔形态[J].中国医学影像技术, 2015, 31(11):1728. [8] 黄淑卿, 张新玲, 吴静.盆底超声在产后康复疗效评估中的应用[J].影像诊断介入放射学, 2015, 24(2):131. [9] 黄淑卿.经会阴超声在围生期的临床应用[J].中国医学影像技术, 2014, 30(9):1432. [10] 王竞宇, 陈艳, 张恩荣, 等.经会阴超声在女性盆底功能障碍性疾病中的应用[J].西部医学, 2013, 25(12):1869. [11] LIU F, XU L, YING T, et al.Three-dimensional ultrasound appearance of pelvic floor in nulliparous women and postpartum women one week after their first delivery[J].Int J Med Sci, 2014, 11(3):234. doi: 10.7150/ijms.7384 -

 点击查看大图
点击查看大图

图(1)表(1)
计量
- 文章访问数: 5072
- HTML全文浏览量: 2351
- PDF下载量: 10
- 被引次数: 0
