

-
颌骨囊肿是临床上比较常见的造成颌骨缺损的疾病,手术摘除颌骨囊肿后所遗留的骨性空腔往往使得创口延期愈合或出现继发性感染[1]。颌骨缺损修复多采用囊腔植骨术和生物材料置入术,但是植骨术的骨来源大多为自体骨,需要开辟第二术区,给病人造成额外痛苦,生物材料置入也会存在一定的排异反应和感染风险[2]。近年来,我科使用富血小板纤维蛋白(platelet-rich fibrin, PRF)联合Bio-Oss骨粉修复颌骨囊肿术后骨缺损取得了良好的临床疗效,现作报道。
-
选取2019年11月至2020年8月于马鞍山市人民医院口腔科收住的颌骨囊肿术后存在一定范围的骨缺损病人共36例,随机分为2组,每组18例。其中观察组男11例,女7例,平均年龄35.24岁;对照组男13例,女5例,平均年龄37.13岁。所有病人的治疗过程符合《赫尔辛基宣言》的要求,并得到了马鞍山市人民医院伦理委员会的批准。术前均告知病人对所接受的治疗、预后及可能出现的并发症情况,病人知情同意并签字为据。纳入标准: (1)年龄≥18周岁,无不良烟酒嗜好,口腔卫生较好,依从性强;(2)颌骨囊肿大小3.0 cm×2.0 cm×1.0 cm~5.0 cm×4.0 cm×3.0 cm,囊肿摘除后呈箱状骨缺损。排除标准: (1)患有糖尿病、骨质疏松等影响骨愈合的全身系统性疾病;(2)颌骨囊肿摘除后呈节段性缺损严重,必须进行自体骨移植,钛板坚强内固定;(3)因自身血液质量不佳,无法制备出足量的PRF。
-
Bio-Oss骨粉(Geistlich Biomaterials,瑞士);海奥生物胶原修复膜(烟台正海生物技术有限公司,中国);Trausim血液离心机及特定配套的采血管、搅拌器及压膜成形器等(江苏创英医疗器械有限公司,中国)。
-
拍摄CBCT测量评估颌骨囊肿大小范围,满足纳入标准的病人予以手术知情告知。术前30 min静脉滴注“头孢呋辛钠”1.5 g,行预防性抗感染治疗。
-
根据术前囊肿大小范围,评估使用不抗凝真空负压采血管的数目并采集病人适量肘部静脉血后迅速放入Trausim血液离心机中,以3 000 r/min的速度离心14 min。离心后可见采血管中血液由上至下分为3层: 血清层、PRF层及红细胞层。打开采血管将血清层倒去,用镊子轻轻夹取黄色胶冻状的PRF置管外,将PRF放入压膜成形器中压制成PRF膜备用(见图 1)。

图 1 PRF的制备
-
常规消毒铺巾,局麻下术区采用角形或梯形切口,切开、翻瓣、去骨,充分暴露囊腔并完整摘除囊肿后,酌情拔除囊肿涉及无法保留的病灶牙。仔细搔刮根尖周围及囊腔骨壁,修整骨创缘后用2%碘酊烧灼骨腔,0.9%氯化钠溶液彻底冲洗。观察组病人将一部分PRF膜剪碎成颗粒状与Bio-Oss骨粉混合搅拌均匀后填入囊肿术后骨缺损空腔内,取PRF膜及海奥生物胶原膜各一份,双层覆盖于骨缺损创面;对照组单纯填入Bio-Oss骨粉,覆盖生物胶原膜。2组病人均对位严密缝合组织瓣,关闭创口。
-
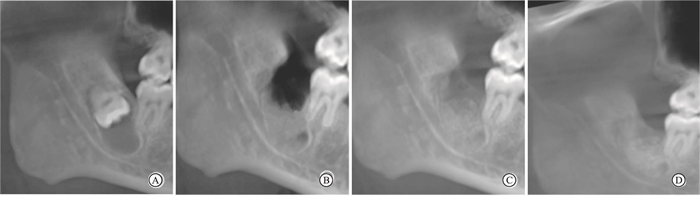
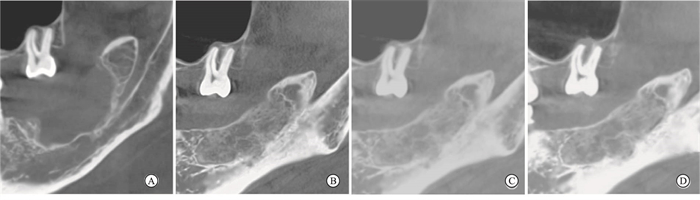
所有病人术后分别于3、6、12个月进行定期随访观察。临床大体观察术区软组织愈合情况,拍摄CBCT影像学观察骨缺损修复情况,通过测量骨缺损区骨密度值,判断2组病人的骨修复情况(见图 2~3)。

图 2 观察组CBCT影像学观察

图 3 对照组CBCT影像学观察
-
采用独立样本t检验。
-
术后2组病人随访观察3~12个月。其中观察组病人术后7 d创口均达到Ⅰ期愈合,CBCT影像学观察病人骨缺损空腔内的充填材料随着时间推移与新生骨及周围骨组织生长良好,可见植骨区与周围正常骨组织的界限和密度逐渐接近,颌骨囊肿术后骨缺损大小范围较术前明显缩小。对照组存在1例病人术后7 d创口轻度糜烂红肿,但未见充填材料排异溢露,经积极抗感染治疗5 d后好转,CBCT影像学观察相比较,术前2组病人骨缺损区骨密度值均较低,差异无统计学意义(P>0.05);观察组术后3、6、12个月骨缺损区骨密度均高于对照组,差异均有统计学意义(P < 0.05~P < 0.01)(见表 1)。
分组 术前 术后3个月 术后6个月 术后12个月 观察组 115.74±22.74 503.46±40.13 587.82±31.83 702.36±30.23 对照组 110.94±20.19 405.24±29.72 461.03±28.87 547.36±35.87 t 0.67 8.34 11.63 14.02 P >0.05 < 0.05 < 0.05 < 0.01 表 1 2组病人骨缺损区骨密度平均值比较(x±s;Hu)
-
牙源性颌骨囊肿非常多见于青壮年颌骨的任何牙位。无论是好发于前牙区的根尖周囊肿,还是好发于后牙区的含牙囊肿或始基囊肿,手术摘除囊肿并拔除病灶牙后所遗留一定大小范围的骨缺损往往难以自行愈合,导致牙槽嵴宽度和高度得不到有效恢复,从而造成颌骨骨量不足影响后期义齿的修复[3]。目前,临床上多采用自体骨移植或人工骨充填的方法来修复颌骨囊肿术后造成一定大小范围的中、大型骨缺损[4]。尤其是近年来,随着种植义齿修复技术的成熟和推广,越来越多的颌骨囊肿术后病人需求种植义齿修复来提高自身的生活质量。
为了促使病人能较快地修复颌骨缺损满足后期种植义齿修复,同时又能避免病人开辟第二术区的痛苦,本研究针对颌骨囊肿术后病人均采用国内外一致好评的Bio-Oss人工骨粉作为修复材料。大量研究已表明Bio-Oss骨粉晶体结构与人体骨的无机成分相似,材料颗粒具有多孔隙,溶解度高,表面性能大,无细胞毒性,生物相容性好的特性[5]。Bio-Oss修复骨缺损的机制在于骨粉颗粒多孔隙结构为成骨细胞提供附着支架,并在其表面沉积,随着骨形成中钙、磷离子缓慢释放,骨粉颗粒逐渐吸收,新骨逐渐钙化形成。虽然Bio-Oss在骨缺损处作为组织工程的支架优势明显,但是该材料只具备骨传导作用,缺乏较强的骨诱导和抗感染能力[6],故制备出一种成骨性能优良的Bio-Oss复合支架材料就显得尤为重要。
研究[7]发现,在颌骨缺损修复中使用自体血小板浓缩物能够提高骨诱导能力,防止创口感染发生从而加快成骨效果形成。PRF制备工艺简单,血液提取后不需要额外添加凝血酶和抗凝剂就可以避免发生交叉感染和排异反应的风险[8-9]。另外PRF还富含大量生长因子、外周血干细胞及免疫细胞,在炎症调节和抗感染方面都发挥了较好的效果[10]。本研究将PRF和Bio-Oss制作成复合材料就是要发挥各自优势,促进范围较大骨缺损的成骨效果。本研究观察组病人术后3个月时已有新骨形成,术后6个月时骨缺损区新生骨面积明显扩大,到术后12个月新生骨组织密度进一步增强,与周围正常骨组织界限趋于模糊,有骨小梁生成。这也再次表明Bio-Oss所具有的三维多孔结构,有利于成骨细胞蔓延生长和毛细血管彼此连通,可以促进成骨细胞黏附和功能代谢[11]。同时,PRF中富含的血小板被激活后释放出转移性生长因子、表皮生长因子和血管内皮细胞生长因子等多种生长因子,一方面对成骨细胞的分化和增殖起着促进作用,另一方面抑制破骨细胞生成功能。这些生长因子之间具有协同效应并与骨形成蛋白相互作用,共同维持着组织环境的平衡,对骨缺损的成骨再生也起着十分重要的作用[12]。我们在临床观察发现,观察组病人的骨密度值明显比对照组高,经统计学数据分析也证实了观察组使用PRF联合Bio-Oss具有良好的促进骨修复效果。可见,随着Bio-Oss表面成骨细胞的聚集和PRF中大量生长因子浓度的提高,促进了成骨细胞增殖、矿化,从而形成有效的骨整合。本研究在Bio-Oss中加入PRF后,使得Bio-Oss材料既具有骨传导性, 又具有骨诱导潜能,能够明显提高成骨效果。
另外,在颌骨缺损空腔内仅仅充填复合人工骨材料是难以达到满意的成骨效果,良好的屏障膜覆盖,无张力严密缝合也至关重要。本研究中使用的口腔修复膜为一种牛皮处理制备的异种脱细胞真皮基质,可诱导成骨细胞贴附,参与生物降解过程,可阻挡牙龈上皮细胞进入骨缺损空腔内,维持成骨细胞生长的三维空间结构,创造出良好的骨再生环境[13]。研究中还充分利用PRF膜中的纤维蛋白属于血管化天然诱导物,有利于营养成分及氧气输入至骨髓干细胞周围,促进分化为成骨细胞的特性[14]。本研究中骨缺损空腔类型多为箱状,四周均有骨壁且唯一的开放创面覆盖屏障膜,能够有效防止咀嚼运动时骨充填材料向四周外溢。我们将PRF凝胶压制成膜,发现PRF膜具有良好的抗剪切性和拉伸强度。为促进骨再生,防止创面感染,所有病人均使用PRF膜覆盖于人工骨材料表面。BORIE等[15]研究就发现在骨增量术中使用PRF膜能够促进口腔软硬组织愈合,减少术后肿痛和感染。本研究对照组病人中有1例出现术区创面轻度红肿糜烂,经病情回溯发现为病人术后进食硬物致创面部分缝线疏松滑脱,再加上口腔卫生保持不佳所致,若创面覆盖PRF膜一定程度上就会减少创面感染的概率。
综上所述,PRF联合Bio-Oss对颌骨囊肿术后骨缺损的修复具有一定的成骨效果,值得在临床上推广及应用。但在临床观察中,我们对如何选取合适的PRF与Bio-Oss的混合比例尚无统一标准,不同年龄段病人的自体血液和颌骨质量也有所差别,这些因素都会影响颌骨缺损修复的作用和疗效。因此PRF联合Bio-Oss修复颌骨囊肿术后骨缺损的稳定性还有待于长时间、大样本观察研究。
富血小板纤维蛋白联合Bio-Oss骨粉修复颌骨囊肿术后骨缺损的疗效
Effects of platelet-rich fibrin combined with Bio-Oss bone substitute in the repair of postoperative bone defect of jaw cyst
-
摘要:
目的观察使用富血小板纤维蛋白(platelet-rich fibrin, PRF)联合Bio-Oss骨粉修复颌骨囊肿术后骨缺损的临床疗效。 方法选取颌骨囊肿术后存在一定大小范围的骨缺损病人共36例作为研究对象,随机分为2组,各18例。对照组病人单纯使用Bio-Oss充填修复骨缺损;观察组病人使用PRF联合Bio-Oss充填颌骨囊肿造成的骨缺损空腔。所有病人术后分别于3、6、12个月进行定期随访观察,通过CBCT影像学检查测量骨密度值评估临床疗效。 结果观察组颌骨囊肿术后伤口愈合良好,对照组有1例术后7 d创口出现轻度糜烂红肿,未见充填材料排异反应。影像学检查显示观察组较对照组病人颌骨缺损空腔内的充填材料随着时间推移与新生骨及周围骨组织生长良好,能够达到临床满意的骨组织修复效果。观察组术后3、6、12个月骨缺损区骨密度均高于对照组,差异均有统计学意义(P < 0.05~P < 0.01)。 结论PRF联合Bio-Oss骨粉可有效提高颌骨囊肿术后骨缺损的成骨疗效。 Abstract:ObjectiveTo observe the clinical efficacy of platelet-rich fibrin(PRF) combined with Bio-Oss bone substitute in the repair of postoperative bone defect of jaw cyst. MethodsA total of 36 patients with bone defects in a certain range after maxillary cyst surgery were randomly divided into the control group and observation group(18 cases in each group).The control group was treated with Bio-Oss filling to repair bone defects, and the observation group was treated with PRF combined with Bio-Oss filling to repair the cavity of bone defect caused by jaw cyst.All patients were regularly followed up for 3, 6 and 12 months after surgery, and the CBCT imaging was used to measure bone mineral density to evaluate the clinical efficacy. ResultsThe wounds of jawbone cyst in the observation group healed well after surgery, 1 case with mild erosion and redness in the control group was identified after 7 days of surgery, and no rejection reaction of filling material was be observed.The results of imaging examination showed that compared with the control group, the filling materials in the cavity of jaw defect in the observation group grew well with the new bone and surrounding bone tissue over time, and the bone tissue repair effect could achieve clinical satisfactory.The bone mineral density in observation group was higher than that in control group at 3, 6 and 12 months after surgery(P < 0.05 to P < 0.01). ConclusionsThe PRF combined with Bio-Oss bone substitute can effectively promote the osteogenic effect of bone defect after maxillary cyst surgery. -
Key words:
- jaw cyst /
- platelet-rich fibrin /
- Bio-Oss bone substitute /
- bone defect
-
表 1 2组病人骨缺损区骨密度平均值比较(x±s;Hu)
分组 术前 术后3个月 术后6个月 术后12个月 观察组 115.74±22.74 503.46±40.13 587.82±31.83 702.36±30.23 对照组 110.94±20.19 405.24±29.72 461.03±28.87 547.36±35.87 t 0.67 8.34 11.63 14.02 P >0.05 < 0.05 < 0.05 < 0.01  下载: 导出CSV
下载: 导出CSV
-
[1] ZHANG ZY. Oral and maxillofacial surgery[M]. 7th ed. Beijing: People's Medical Publishing House, 2012: 177. [2] ZHOU J, DU RH. Assessment on the treatments for cyst of the jaws[J]. J Oral Maxillofac Surg, 2012, 22(4): 229. [3] CHIAPASCO M, ROSSI A, MOTTA JJ, et al. Spontaneous bone regeneration after enucleation of large mandibular cysts: a radiographic computed analysis of 27 consecutive cases[J]. J Oral Maxillofac Surg, 2000, 58(9): 942. doi: 10.1053/joms.2000.8732 [4] AKRAM M, FAROOQ FM, SHAHZAD ML, et al. A comparison of treating unicameral bone cyst using steroids and percutaneous autologous bone marrow aspiration injection[J]. J Pak Med Assoc, 2015, 65(11 Suppl 3): S156. [5] 王国世, 李韶伟, 蔡露. 牙种植采用引导骨再生术Bio-oss吸收的定量分析[J]. 上海口腔医学, 2012, 21(3): 317. [6] SIVOLELLA S, BRESSAN E, SALATA LA, et al. Deproteinized bovine bone mineral particles and osseointegration of implants without primary bone contact: an experimental study in dogs[J]. Clin Oral Implants Res, 2014, 25(3): 296. doi: 10.1111/clr.12154 [7] AMIT A. Evolution current status and advances in application of platelet concentrate in periodontics and implantology?[J]. World J Clin Cases, 2017(5): 159. [8] DOHAN DM, CHOUKROUN J, DISS A, et al. Platelet-rich fibrin(PRF): a second-generation platelet concentrate. Part Ⅲ: leucocyte activation: a new feature for platelet concentrates[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2006, 101(3): e51. doi: 10.1016/j.tripleo.2005.07.010 [9] 方冬冬, 后军, 杨全全, 等. 富血小板纤维蛋白复合骨诱导在颌骨缺损中的应用疗效[J]. 安徽医学, 2016, 37(7): 868. [10] 周延民, 付丽. 富血小板纤维蛋白在口腔软硬组织再生中的作用——回顾与展望[J]. 口腔医学, 2018, 38(11): 961. [11] SHAH R, THOMAS R, MEHTA DS. An update on the protocols and biologic actions of platelet rich fibrin in dentistry[J]. Eur J Prosthodont Restor Dent, 2017, 25(2): 64. [12] AZITA T, HOSSEIN B, FEREYDOUN P, et al. The effect of autologous leukocyte platelet rich fibrin on the rate of orthodontic tooth movement: a prospective randomized clinical trial[J]. World J Clin Cases, 2017(5): 159. [13] DEYHIMI P, RAZAVI SM, SHAHNASERI S, et al. Rare and extensive malignant melanoma of the oral cavity: report of two cases[J]. J Dent (Shiraz), 2017, 18(3): 227. [14] RAY H, MARCELINO J, BRAGA R, et al. Long-term follow up of revascularization using platelet-rich fibrin[J]. Dental Traumatol, 2016, 32(1): 80. [15] BORIE E, OLIVI D, ORSI IA, et al. Platelet-rich fibrin application in dentistry: a literature review[J]. Int J Clin Exp Med, 2015, 8(5): 7922. -

 点击查看大图
点击查看大图

图(3)表(1)
计量
- 文章访问数: 2496
- HTML全文浏览量: 1297
- PDF下载量: 2
- 被引次数: 0
