

-
牙周病是一种发生在牙龈、牙槽骨、牙周膜等牙齿支持组织的慢性、进行性、破坏性的口腔疾病,包括牙周炎和牙龈病两大类,临床常主诉为口腔异味、刷牙出血、咬合疼痛、牙龈肿胀、牙齿松动、食物嵌塞等[1-2]。我国第三次口腔健康流行病学调查显示老年人中仅有14.1%的牙周处于健康状态, 老年人由于自身免疫力和修复能力下降,对疾病认知也相对缺乏,故是牙周病的高发人群[3]。牙周病病程较长,早期由于病情较轻,无自觉症状或症状不明显易被忽视。当病情逐渐加重化,病人有明显症状时往往已进入晚期,此时牙周组织严重萎缩,甚至无法治疗而做拔除处理,不仅严重影响病人的生活质量,还有可能增加病人全身共病的发病风险,故如何预测和控制病情的发展对牙周病病人预后尤其重要[4-5]。目前国内外已就牙周病的多因素致病性展开了大量探究,但尚未能进一步构建可有效预测牙周病严重程度的模型[6-7]。列线图是一种基于多因素回归模型,由风险指标及其对应的带有刻度的线段组成的可视化模型,近年来被临床广泛应用于预测风险事件[8-9]。基于此,本研究拟分析老年牙周病病人病情严重程度的影响因素,并在此基础上建立相关列线图预测模型,旨在为临床控制老年牙周病病情进展、改善病人预后提供参考依据。
-
选取2018年9月至2020年9月于我院就诊的老年牙周病病人作为研究对象。纳入标准:(1)年龄≥60岁;(2)均符合牙周病的诊断标准[10];(3)口腔余留牙数≥16颗且磨牙数≥4颗;(4)近一年内未进行过牙周治疗。排除标准:(1)无牙颌;(2)合并心肺肝肾等重要器官功能障碍;(3)近3个月内服用过抗菌药物或非甾体抗炎药;(4)合并精神疾病。病人均知情同意,本研究经我院伦理委员会审批通过。共纳入279例病人,年龄60~81岁,平均(70.16±8.25)岁。采用整群随机分组法将病人分为训练集(n=213)和验证集(n=66)。
-
采用Hufriedy刻度探针对受试者进行口腔检查,包括探诊出血、探诊深度和附着丧失。牙槽骨吸收通过影像学检查完成。
-
轻度:探诊深度≤4 mm,且附着丧失 < 3 mm,影像学提示牙齿松动 < Ⅱ~Ⅲ度,牙槽骨吸收未超过根长的1/3。中重度:探诊深度>4 mm,或附着丧失≥3 mm,影像学提示牙齿松动超过Ⅱ~Ⅲ度,牙槽骨吸收至少为根长的1/3[11]。
-
经病人知情同意后,向其发放由我院自行设计的调查问卷,规定统一指导语,嘱咐并协助病人按照自身实际情况填写,填写完毕后收回。问卷内容具体包括:性别、年龄、体质量指数(body mass index,BMI)、文化程度、居住地、是否吸烟、是否饮酒、有无糖尿病、有无冠心病、有无高血压、有无高血脂、有无拔牙史、有无义齿、是否偏侧咀嚼、刷牙频率和是否定期口腔检查。本次研究共发放问卷279份,回收率100%,合格率100%。
-
采用χ2检验和多因素logistic回归分析。采用R(R3.5.3)软件包和rms程序包建立列线图模型。采用Bootstrap法做内部验证,外部验证通过验证集完成,模型的预测能力采用一致性指数(C-index)、校正曲线和ROC曲线进行评价。
-
279例病人中探诊出血阳性者为275例,轻度牙周病83例(29.7%),中重度牙周病196例(70.3%)。
-
轻度牙周病病人69例(轻度组),中重度牙周病病人144例(中重度组),对比2组资料,结果显示:中重度组病人年龄≥70岁、吸烟、糖尿病、偏侧咀嚼和刷牙频率 < 2次/天者多于轻度组,差异有统计学意义(P < 0.01)(见表 1)。
因素 轻度组(n=69) 中重度组(n=144) χ2 P 性别 < 男 41 98 1.53 >0.05 < 女 28 46 年龄/岁 < < 70 47 65 9.88 < 0.01 < ≥70 22 79 BMI/(kg/m2) < 24 55 113 0.04 >0.05 ≥24 14 31 文化程度 小学及以下 43 97 中学 20 34 0.72 >0.05 专科及以上 6 13 居住地 农村 41 76 0.83 >0.05 城镇 28 68 吸烟 24 82 9.17 < 0.01 饮酒 28 57 0.02 >0.05 糖尿病 5 35 8.90 < 0.01 冠心病 11 27 0.25 >0.05 高血压 16 31 0.08 >0.05 高血脂 11 23 0.00 >0.05 拔牙史 6 13 0.01 >0.05 义齿 有 7 21 0.81 >0.05 无 62 123 偏侧咀嚼 27 85 7.41 < 0.01 刷牙频率/(次/天) < 2 21 74 8.29 < 0.01 ≥2 48 70 定期口腔检查 是 10 19 0.07 >0.05 否 59 125 表 1 老年牙周病病人病情进展至中重度的单因素分析
-
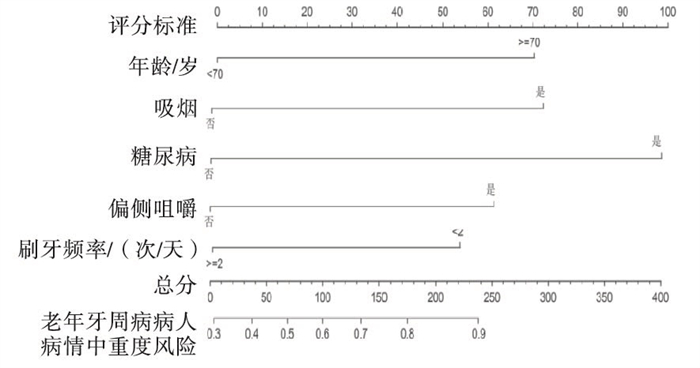
以老年牙周病病人病情严重程度为因变量(中重度=1,轻度=0),以中重度组和轻度组单因素分析中有统计学意义的5个项目[年龄(≥70岁=1, < 70岁=0);吸烟(是=1,否=0);糖尿病(是=1,否=0);偏侧咀嚼(是=1,否=0);刷牙频率(< 2次/天=1,≥2次/天=0)]为自变量,进行二分类logistic回归分析,结果显示:年龄≥70岁、吸烟、糖尿病、偏侧咀嚼、刷牙频率 < 2次/天是老年牙周病病人病情进展至中重度的独立危险因素(P < 0.05~P < 0.01)(见表 2)。
项目 B SE Waldχ2 P OR(95%CI) 年龄(≥70岁) 0.910 0.334 7.45 < 0.01 2.485(1.292~4.778) 吸烟(是) 0.952 0.330 8.33 < 0.01 2.591(1.357~4.946) 糖尿病(是) 1.294 0.529 5.99 < 0.05 3.648(1.294~10.284) 偏侧咀嚼(是) 0.814 0.324 6.32 < 0.05 2.257(1.197~4.258) 刷牙频率(< 2次/天) 0.710 0.334 4.52 < 0.05 2.034(1.057~3.916) 常量 -0.960 0.338 8.09 < 0.01 0.383(-) 表 2 老年牙周病病人病情进展至中重度的多因素logistic回归分析
-
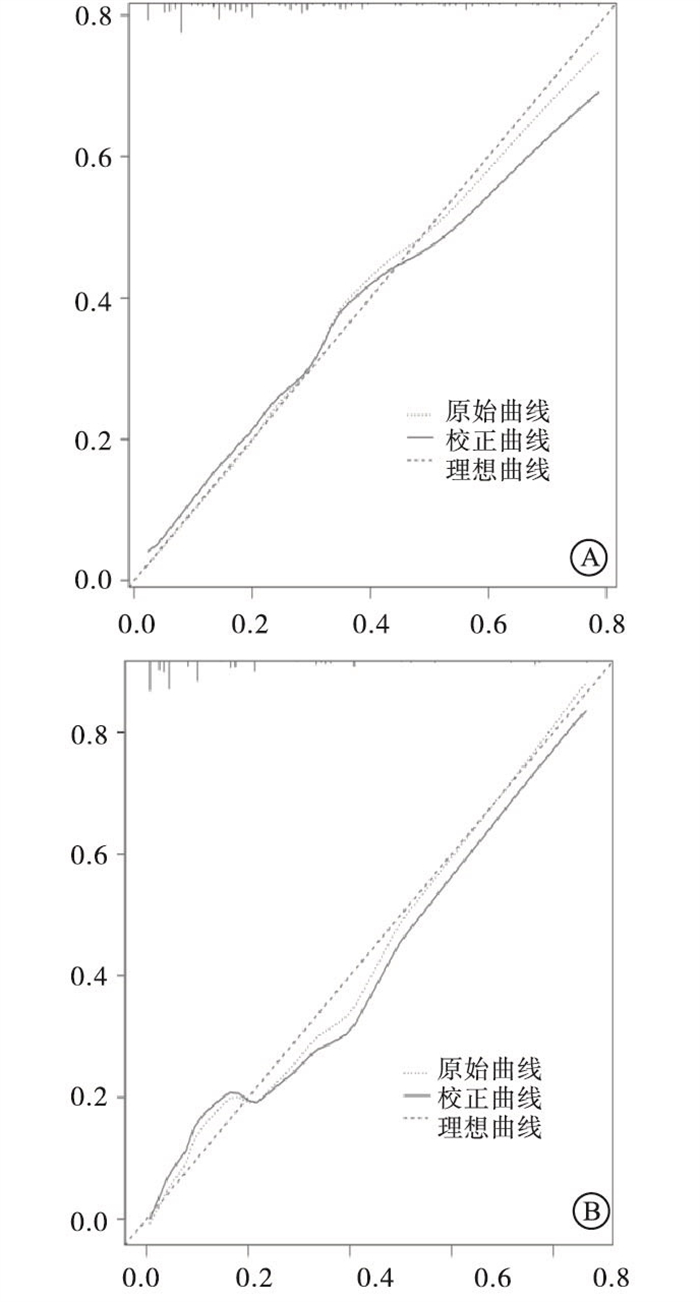
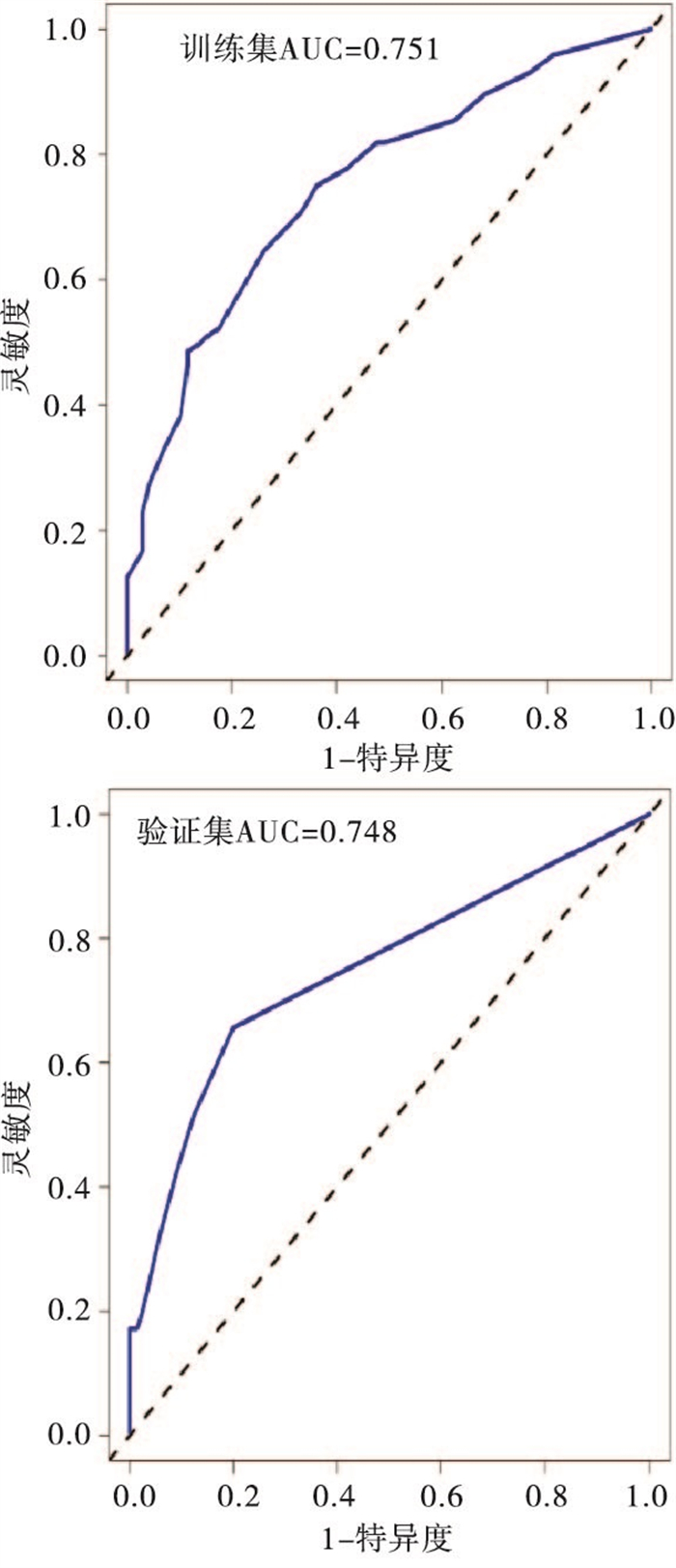
本研究基于筛选出的5项独立危险因素建立了预测老年牙周病病人病情进展至中重度的列线图模型(见图 1)。模型验证结果显示:训练集和验证集的C-index分别为0.734(95%CI:0.712~0.758)和0.717(95%CI:0.698~0.738);两集的校正曲线和理想曲线拟合反映均较好(见图 2);两集的ROC曲线下面积(AUC)分别为0.751和0.748(见图 3)。

图 1 预测老年牙周病病人病情进展至中重度的列线图风险模型

图 2 列线图模型的校正曲线

图 3 列线图模型的ROC曲线
-
牙周病是一种分布较广、病因复杂的慢性感染疾病,轻度牙周病仅表现为牙龈出血,病变局限在游离龈和龈乳头。牙槽骨吸收的程度与炎症的时间和严重程度有关,病情进展至中重度可出现牙齿逐渐松动、移位,继而导致牙齿丧失,且牙齿丧失的数目常不是单个,多数牙甚至全口牙同时受累,故中重度牙周病对人类口腔健康具有巨大的威胁[12]。本次研究结果显示279例老年牙周病病人中中重度多达196例(70.3%),可见病人就诊时病情大多已较为严重,故及时了解并掌握相关危险因素对牙周病病情控制和预防至关重要。
本研究结合老年牙周病病人的参数资料筛选出年龄≥70岁、吸烟、糖尿病、偏侧咀嚼、刷牙频率 < 2次/天是老年牙周病病人病情进展至中重度的独立危险因素(P < 0.05~P < 0.01)。李理等[13]报道年龄是牙周病病人病情加重的危险因素,本文结果与之一致。老年人随着年龄的增长,自身免疫力下降,结缔组织的新陈代谢衰退,易受到病原菌侵袭致使牙周正常菌群的动态平衡被破坏。同时,唾液腺随着时间推移会发生退行性改变,导致唾液分泌减少,易造成食物残渣滞留在牙周组织上而发生菌斑推挤,加重牙周病情。JEONG等[14]报道吸烟者的牙周病患病率是非吸烟者的2.17倍,本研究也显示吸烟的老年牙周病病人病情进展至中重度的风险更高。分析原因可能是由于吸烟会造成病人口腔内环境变差,局部血液循环受阻,氧量降低,为厌氧菌的生长繁殖提供了有利条件,从而增加了致病菌侵袭的风险,导致牙菌斑、牙石堆积增多,牙槽骨吸收加快,牙周病症加重。同时,FATEMI等[15]还指出吸烟可使牙周组织对TLR-4的表达水平增加,导致免疫细胞对致病菌的识别增强,从而促进炎症反应,在破坏病原菌的同时也损伤了牙周组织。既往研究[16-17]显示糖尿病是牙周病严重程度的危险因素,本文结果与之一致。究其原因,可能是由于糖尿病病人牙周组织含糖量较高,为致病菌的生长创造了有利条件。此外,糖尿病会增强糖化末端产物与受体的作用,造成白细胞、血管基底膜、周围神经等出现病理性改变,导致病人免疫力下降,更容易引起致病菌感染,且愈合缓慢,从而加重牙周病情。牙周病病人往往由于牙齿疼痛或不适失用患侧牙齿,使得单侧咀嚼频率增加,长时间形成偏侧咀嚼的习惯。姚巍等[18]报道不同程度的牙周病病人偏侧咀嚼情况存在统计学差异,本文与之一致。偏侧咀嚼会导致磨牙牙合面的磨耗不一致,咀嚼侧咀嚼压力增强,可引起牙周膜结构致密、宽度增加,而失用侧牙齿因缺乏自洁作用可形成软垢和牙结石,加重牙周病情。曲梦等[19]报道牙周炎严重程度与病人口腔健康素养水平呈负相关,本研究中显示刷牙频率 < 2次/天的牙周病病人病情为中重度的风险更高,刷牙是一种简单有效的机械性菌斑控制方法,可祛除软垢、食物残渣,抑制牙周微生物的生长繁殖。刷牙还可通过按摩牙龈增进局部血液循环,增强牙周组织对局部刺激的防御能力,维护口腔健康卫生。
本次研究结合logistic回归的筛选结果构建了老年牙周病病人病情进展至中重度的列线图预测模型。相较于专家[20]提出的牙周病预测指标Charlson共病指数和TONETTI等[21]报道的用于区别牙周诊断的经验决策算法,本次列线图模型在实际使用中免去了繁杂的代数运算,具有可视可读、理解记忆简单、应用方便快捷等优势。同时,在对列线图预测效能的验证中,为避免模型过度拟合,本研究采用C-index对模型的预测情况和实际情况进行了评估,结果显示训练集和验证集分别为0.734(95%CI:0.712~0.758)和0.717(95%CI:0.698~0.738),同时,训练集校正曲线也显示与理想曲线贴合度良好,预测值同实测值基本一致,但在验证集中校正曲线浮动于理想曲线两侧,存在一定偏差,可能与样本量不足和变量偏倚性选择有关,但可见此次列线图模型在具有良好的预测准确性。此外,模型的ROC曲线还显示两集的AUC分别为0.751和0.748,表明列线图兼具良好的区分度。临床使用人员可依据列线图中的危险指标收集病人资料,个体化预测老年牙周病病人病情中重度的风险,并进行危险分层,针对高风险病人应做到及时诊断和及早治疗,旨在减轻牙周病的严重程度,控制其发展。对于已是中重牙周病病人,应按症给予药物治疗或深袋刮治术、龈切除术等手术治疗,尽可能抑制病情进一步恶化。此外,针对可控危险指标,临床应对牙周病病人进行口腔健康教育和指导,建立良好的口腔卫生习惯,如戒烟或减少吸烟频率,改正单侧咀嚼的恶习,至少早晚各刷牙一次,以达到清除菌斑和其他有害刺激因子的目的,同时提高宿主的抵抗能力,改善牙周病预后。
综上所述,年龄≥70岁、吸烟、糖尿病、偏侧咀嚼、刷牙频率 < 2次/天是老年牙周病病人病情进展至中重度的独立危险因素,基于危险因素建立的列线图模型能够较好地预测老年牙周病病人病情的严重程度,有助于临床筛查中重度牙周病病人和改进治疗方法。本次研究的局限性在于取自单中心的样本量有限,代表性不足,且在变量的选择上存在一定程度的选择性偏倚,未能纳入饮食习惯、个人卫生习惯、刷牙时间、服用药物等指标,故模型仍需多中心、大样本、更细化纳入变量的研究予以进一步完善。
个体化预测老年牙周病病人病情严重程度的风险列线图模型的建立与验证
Establishment and validation of risk nomogram model for individual prediction of severity of periodontal disease in elderly patients
-
摘要:
目的构建可个体化预测老年牙周病病人病情严重程度的风险列线图模型,并对模型的预测效能进行验证。 方法选取279例老年牙周病病人作为研究对象,收集病人相关资料,采用单因素和logistic回归多因素分析影响老年牙周病病人病情进展至中重度的相关因素,并建立列线图预测模型。 结果279例中,轻度83例(29.7%),中重度196例(70.3%)。年龄≥70岁、吸烟、糖尿病、偏侧咀嚼、刷牙频率 < 2次/天是老年牙周病病人病情进展至中重度的独立危险因素(P < 0.05~P < 0.01)。基于以上5项危险因素建立相关列线图模型,并对该模型进行验证。结果显示:训练集和验证集的C-index分别为0.734(95%CI:0.712~0.758)和0.717(95%CI:0.698~0.738),两集的校正曲线和理想曲线拟合反映均较好,两集的AUC分别为0.751和0.748。 结论老年牙周病病人病情进展至中重度的危险因素较多,本研究基于危险因素建立的列线图模型具有良好的预测能力,可为临床早期控制牙周病病情发展提供参考依据。 Abstract:ObjectiveTo construct a risk nomogram model for predicting the severity of periodontal disease in elderly patients, and to verify the predictive efficacy of the model. MethodsA total of 279 elderly patients with periodontal disease were selected as the research objects, and the relevant data of the patients were collected.Univariate logistic regression was used to analyze the related factors affecting the progression of the elderly patients with periodontal disease to moderate to serve level, and the nomogram prediction model was established. ResultsAmong the 279 cases, 83 cases (29.7%) were mild, 196 cases (70.3%) were moderate and severe.Age ≥70 years old, smoking, diabetes mellitus, unilateral chewing, brushing frequency < 2 times/d were the independent risk factors for the progression of moderate to severe periodontal disease in elderly patients (P < 0.05 to P < 0.01).Based on the above five risk factors, the relevant nomogram model was established and verified.The results showed that the C-index of training set and validation set were 0.734 (95%CI: 0.712-0.758) and 0.717 (95%CI: 0.698-0.738), respectively.The calibration curve and ideal curve fitting of the two sets were well reflected, and the AUC of the two sets were 0.751 and 0.748, respectively. ConclusionsThere are many risk factors for the progression of periodontal disease in elderly patients.The nomogram model based on risk factors has good predictive ability, which can provide reference for early clinical control of periodontal disease. -
Key words:
- periodontal disease /
- elderly patients /
- disease severity /
- risk factors /
- nomogram
-
表 1 老年牙周病病人病情进展至中重度的单因素分析
因素 轻度组(n=69) 中重度组(n=144) χ2 P 性别 < 男 41 98 1.53 >0.05 < 女 28 46 年龄/岁 < < 70 47 65 9.88 < 0.01 < ≥70 22 79 BMI/(kg/m2) < 24 55 113 0.04 >0.05 ≥24 14 31 文化程度 小学及以下 43 97 中学 20 34 0.72 >0.05 专科及以上 6 13 居住地 农村 41 76 0.83 >0.05 城镇 28 68 吸烟 24 82 9.17 < 0.01 饮酒 28 57 0.02 >0.05 糖尿病 5 35 8.90 < 0.01 冠心病 11 27 0.25 >0.05 高血压 16 31 0.08 >0.05 高血脂 11 23 0.00 >0.05 拔牙史 6 13 0.01 >0.05 义齿 有 7 21 0.81 >0.05 无 62 123 偏侧咀嚼 27 85 7.41 < 0.01 刷牙频率/(次/天) < 2 21 74 8.29 < 0.01 ≥2 48 70 定期口腔检查 是 10 19 0.07 >0.05 否 59 125  下载: 导出CSV
下载: 导出CSV
表 2 老年牙周病病人病情进展至中重度的多因素logistic回归分析
项目 B SE Waldχ2 P OR(95%CI) 年龄(≥70岁) 0.910 0.334 7.45 < 0.01 2.485(1.292~4.778) 吸烟(是) 0.952 0.330 8.33 < 0.01 2.591(1.357~4.946) 糖尿病(是) 1.294 0.529 5.99 < 0.05 3.648(1.294~10.284) 偏侧咀嚼(是) 0.814 0.324 6.32 < 0.05 2.257(1.197~4.258) 刷牙频率(< 2次/天) 0.710 0.334 4.52 < 0.05 2.034(1.057~3.916) 常量 -0.960 0.338 8.09 < 0.01 0.383(-)
下载: 导出CSV
-
[1] HUANG K, MATSUDA K, IWAKABE K, et al. Association between oral health behavior and periodontal disease among Korean adults: the Korea national health and nutrition examination survey[J]. Medicine, 2017, 96(7): e6176. doi: 10.1097/MD.0000000000006176 [2] 武峻捷, 廖圣恺, 韩前乾, 等. 安徽省医学院校大学生口腔健康知识、态度、行为分析[J]. 蚌埠医学院学报, 2021, 46(1): 131. [3] 齐小秋. 第三次全国口腔健康流行病学调查报告[M]. 北京: 人民卫生出版社, 2008: 46. [4] REYNOLDS I, DUANE B. Periodontal disease has an impact on patients' quality of life[J]. Evid Based Dent, 2018, 19(1): 14. doi: 10.1038/sj.ebd.6401287 [5] ZHAO D, ZHEN Z, PELEKOS G, et al. Periodontal disease increases the risk for onset of systemic comorbidities in dental hospital attendees: an 18-year retrospective cohort study[J]. J Periodontol, 2018, 90(3): 225. [6] 杜娟, 段春红. 老年人群牙周疾病危险因素分析[J]. 中国药物与临床, 2018, 7(18): 11312. [7] PHAM TAV, KIEU TQ, NGO LTQ. Risk factors of periodontal disease in Vietnamese patients[J]. J Investig Clin Dent, 2018, 9(1): e12272. doi: 10.1111/jicd.12272 [8] STROBEL O, BVCHLER MW. A nomogram for the prediction of malignancy in branch-duct IPMN[J]. Chirurg, 2019, 90(Suppl 2): 92. [9] HE CB, MAO YZ, WANG J, et al. Nomograms predict long-term survival for patients with periampullary adenocarcinoma after pancreatoduodenectomy[J]. BMC Cancer, 2018, 18(1): 327. doi: 10.1186/s12885-018-4240-x [10] CATON JG, ARMITAGE G, BERGLUNDH T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions-introduction and key changes from the 1999 classification[J]. J Clin Periodontol, 2018, 45 Suppl 20: S1. [11] 中华口腔医学会牙周病学专业委员会. 重度牙周炎诊断标准及特殊人群牙周病治疗原则的中国专家共识[J]. 中华口腔医学杂志, 2017, 52(2): 67. [12] 林彦君, 周勇, 林继超, 等. 重度牙周炎患者种植修复时机的考量[J]. 口腔医学, 2019, 39(10): 944. [13] 李理, 杨介平, 刘伟, 等. 影响慢性牙周炎患者病情严重程度的危险因素Logistics回归分析[J]. 解放军预防医学杂志, 2018, 36(1): 110. [14] JEONG W, CHOI DW, KIM YK, et al. Associations of electronic and conventional cigarette use with periodontal disease in South Korean adults[J]. J Periodontol, 2020, 91(1): 55. doi: 10.1002/JPER.19-0060 [15] FATEMI K, RADVAR M, REZAEE A, et al. Comparison of relative TLR-2 and TLR-4 expression level of disease and healthy gingival tissue of smoking and non-smoking patients and periodontally healthy control patients[J]. Aust Dent J, 2013, 58(3): 315. doi: 10.1111/adj.12089 [16] SIMON L, TOBEY M, WILSON M, et al. Feasibility of integrating a dental hygienist into an inpatient medical team for patients with diabetes mellitus[J]. J Public Health Dent, 2019, 79(3): 188. doi: 10.1111/jphd.12320 [17] OBERTI L, GABRIONE F, NARDONE M, et al. Two-way relationship between diabetes and periodontal disease: a reality or a paradigm?[J]. J Biol Regul Homeost Agents, 2019, 33(3 Suppl. 1): 153. [18] 姚巍, 张鸿军, 周水华. 老年人牙周病病情严重程度的影响因素及预防策略[J]. 海南医学, 2020, 31(1): 86. [19] 曲梦, 王玲芳, 郭伟伟, 等. 牙周炎患者口腔健康素养与疾病严重程度的相关性分析[J]. 中华现代护理杂志, 2019, 25(6): 770. [20] LEE JH, CHOI JK, JEONG SN, et al. Charlson comorbidity index as a predictor of periodontal disease in elderly participants[J]. J Periodontal Implant Sci, 2018, 48(2): 92. doi: 10.5051/jpis.2018.48.2.92 [21] TONETTI MS, SANZ M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education[J]. J Clin Periodontol, 2019, 46(4): 398. doi: 10.1111/jcpe.13104 -

 点击查看大图
点击查看大图
图(3)表(2)
计量
- 文章访问数: 2871
- HTML全文浏览量: 1520
- PDF下载量: 5
- 被引次数: 0
