

-
自然分娩产后出血(postpartum hemorrhage,PPH)是指产妇在分娩后24 h内阴道失血量≥500 mL,属产科危重并发症[1]。随我国生育政策放宽,高龄追生现象及妊娠期各种并发症明显增多,使得PPH高危因素较以往有明显变化,导致以往一些PPH预测评分表内容不能适应目前生育人群结构的变化。PPH的突发性不仅会引起感染、贫血,失血过多还可引起弥散性血管内凝血、失血性休克等并发症,甚至增加产妇死亡风险[2]。然而,目前关于PPH危险因素的研究都是基于一些分娩过程中的指标进行[3-4],缺乏结合孕妇临产前指标。本研究结合孕妇临产前指标并整合近年孕妇分娩后发生PPH的各危险因素,构建有效的预测模型,为临床早期评估可能发生PPH的高风险孕妇提供参考。现作报道。
-
选择2020年3月至2021年5月在我院产科进行产检并最终阴道分娩的3 067例产妇作为研究对象。纳入标准:(1)年龄≥20岁;(2)产妇的人口学特征、产检信息完整;(3)孕周≥37周。排除标准:(1)合并严重性器质性疾病;(2)合并恶性肿瘤;(3)凶险性前置胎盘;(4)胎儿严重畸形;(5)分娩前3个月存在外伤、感染或手术;(6)产道异常。以产妇阴道分娩后24 h内是否发生PPH分为PPH组(n=229)和非PPH组(n=2 838)。
-
收集产妇一般资料,包括年龄、孕次、产次、孕周、胎数、剖宫产史,妊娠期并发症,如妊娠期糖尿病、妊娠期高血压疾病(妊高症)等,胎盘情况,临产前血液指标如血红蛋白(hemoglobin,Hb)、D-二聚体、凝血酶原时间(prothrombin time,PT)、活化部分凝血活酶时间(activated partial thromboplastin time,APTT)、凝血酶时间(thrombin time,TT)、纤维蛋白原(fibrinogen,Fib),以及产程、胎儿体质量、产后出血情况等。
-
采用容积法和称重法测量产妇分娩后24 h内的出血量,即胎儿经阴道分娩出后,将带有刻度的接血容器置于产妇臀收集血液,直至产后2 h取出接血容器,记录接血容器的血量刻度;敷料及纱布中的出血量采用重法测量,即失血量(mL)=[湿垫/纱布质量(g)-干垫/纱布质量(g)]/1.05。二者相加即为产后24 h内产妇出血量。参照《妇产科学》产后出血诊断标准[5],当阴道流血量≥500 mL则定义为产后出血。
-
采用t检验和χ2检验,多因素分析采用二元logistic回归分析。采用R语言(R3.4.3)软件绘制列线图,通过rms程序包建立列线图预测模型及校准曲线,通过受试者工作特征曲线(ROC)下的AUC面积评估列线图模型效能,并采用Bootstrap法自采样1 000次抽样对列线图模型的预测能力进行验证。
-
PPH组与非PPH组的年龄、多胎、妊高症、临产前D-二聚体、临产前Fib、第三产程时间、胎盘粘连、胎儿体质量指标的比较差异均有统计学意义(P < 0.01)(见表 1)。
分组 n 年龄/岁 孕次 产次 孕周/周 多胎 剖宫产史 妊高症 妊娠期糖尿病 临产前Hb/(g/L) 临产前D-二聚体/(mg/L) PPH组 229 29.38±3.50 1.39±0.38 1.12±0.31 39.42±1.76 13 39 34 16 124.75±16.43 0.45±0.12 非PPH组 2 838 27.22±3.11 1.36±0.41 1.10±0.28 39.34±1.83 67 396 158 131 126.39±17.34 0.43±0.09 t — 10.01 1.07 1.03 0.64 6.53* 1.65* 31.10* 2.61* 1.38 3.14 P — < 0.01 >0.05 >0.05 >0.05 < 0.01 >0.05 < 0.01 >0.05 >0.05 < 0.01 分组 n 临产前PT/s 临产前APTT/s 临产前TT/s 临产前Fib/(g/L) 第一产程/min 第二产程/min 第三产程/min 胎盘粘连 胎儿体质量/kg PPH组 229 10.89±0.92 31.78±2.95 12.71±1.27 4.03±0.58 6 003.57±190.54 80.21±25.16 10.22±3.32 27 3.33±0.73 非PPH组 2 838 11.01±1.05 32.07±2.86 12.86±1.75 4.59±0.62 5 989.75±192.95 77.98±24.37 7.83±2.15 156 3.15±0.58 t — 1.68 1.47 1.27 13.21 1.04 1.33 15.41 14.96* 4.42 P — >0.05 >0.05 >0.05 < 0.01 >0.05 >0.05 < 0.01 < 0.01 < 0.01 *示χ2值 表 1 2组的临床资料比较(x±s)
-
以孕妇自然分娩后是否(0=否;1=是)发生PPH为因变量,将表 1分析有统计学意义(P < 0.05)的因素作为自变量,对分类资料进行赋值[多胎(0=否;1=是)、妊高症(0=无;1=有)、胎盘粘连(0=无;1=有)],计量资料(年龄、临产前D-二聚体、临产前Fib、第三产程时间、胎儿体质量)以实际值录入。多因素logistic回归分析显示,年龄高、多胎、有妊高症、临产前D-二聚体升高、第三产程时间长、有胎盘粘连、胎儿体质量大均是孕妇自然分娩发生PPH的危险因素(P < 0.01),临产前Fib升高为孕妇自然分娩发生PPH的保护因素(P < 0.01)(见表 2)。
变量 B SE Waldχ2 P OR(95%CI) 年龄 0.39 0.032 153.04 < 0.01 1.481(1.391~1.576) 多胎 1.76 0.414 18.12 < 0.01 5.825(2.588~13.114) 妊高症 1.07 0.251 18.26 < 0.01 2.927(1.788~4.790) 临产前D-二聚体 2.59 0.873 8.80 < 0.01 13.305(2.405~73.599) 临产前Fib -2.62 0.180 213.22 < 0.01 0.073(0.051~0.103) 第三产程时间 0.05 0.014 13.07 < 0.01 1.054(1.04~1.084) 胎盘粘连 0.77 0.271 8.06 < 0.01 2.155(1.268~3.662) 胎儿体质量 0.72 0.133 29.15 < 0.01 2.048(1.579~2.657) 表 2 多因素logistic分析结果
-
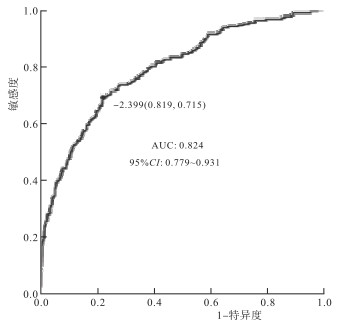
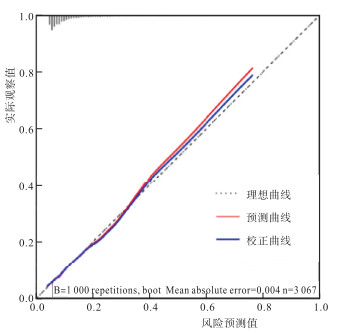
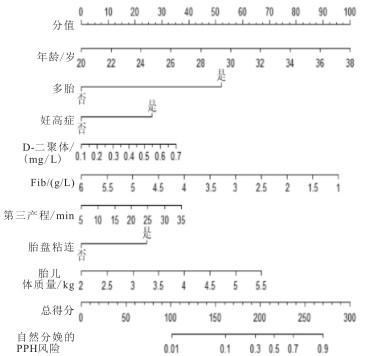
列线图模型依据表 2所筛选出的8个影响因素进行构建(见图 1)。内部验证发现,列线图模型预测孕妇自然分娩PPH的AUC为0.824,灵敏度为0.819,特异度为0.715,提示列线图模型的区分能力较好(见图 2)。拟合优度(Hosmer-Lemeshow)偏差性检验模型预测值与实际值之间的偏差性不具备统计学意义(χ2=5.07,P < 0.05),表明预测模型不存在过拟合现象。经Bootstrap法自1 000次抽样对列线图模型的验证发现校准曲线的MAE为0.004,说明校正曲线与理想曲线贴合良好,模型预测值与实际发生值具有良好的一致性(见图 3)。

图 1 孕妇自然分娩的PPH风险预测列线图模型

图 2 列线图模型预测孕妇自然分娩PPH的ROC曲线分析

图 3 列线图模型预防孕妇自然分娩PPH的校正图
-
PPH的发生涉及子宫收缩、胎盘因素、妊娠期并发症、凝血机制等诸多因素,每个影响因素的机制不尽相同,且这些因素可并存,可互为因果、相互作用、相互影响,形成恶性循环[6]。因此,早期区分和鉴别可能出现PPH高风险人群,有利于早期采取措施来降低或避免PPH所带来的危害。
本研究分析自然分娩产妇的临床信息发现年龄、多胎、妊高症、临产前D-二聚体、临产前Fib、第三产程时间、胎盘粘连、胎儿体质量与PPH相关。其原因为(1)随年龄增长,孕产妇生殖系统机能下降,如子宫肌纤维呈退行性下降,使得分娩时弹力不足,子宫收缩能力下降,常常导致缩宫素用量不足,使得子宫血窦持续开放引起出血不止。VALDES等[7]分析2 136例产妇资料,发现年龄是PPH的危险因素,本研究结果与之相符。(2)随着辅助生殖技术普及,多胎妊娠明显增多。多胎孕妇子宫膨胀过度,加大子宫纤维的拉伸,影响子宫收缩,造成宫缩乏力,增加出血概率。金洪运等[8]报道多胎妊娠是PPH的影响因素,本研究结果与之相符。(3)妊高症是妊娠期以血压升高为基本表现的一系列疾病。血压升高所引起的血压变异波动,其产生的剪切力对血管壁具有破坏性作用,可增加血管内皮损伤,导致子宫小动脉痉挛[9],致使子宫局部缺血,易发生继发性溶血,加重产妇分娩后的出血量。(4)机体凝血与纤溶过程均属正常的保护性生理反应,其能确保血管通畅,预防血液流失过多。D-二聚体浓度特异性增加,会促进血栓形成,导致纤维蛋白溶解,增加出血风险。张颖等[10]研究证实D-二聚体对产妇PPH具有较高的预测价值。妊娠过程中滋养叶的碎片通过血液进入循环系统,致使血管内呈现凝血现象等[11],激活纤溶系统,进而增加PPH倾向。(5)出血导致凝血物质消耗所引起的继发性凝血功能紊乱是加重PPH的重要因素[12]。Fib则是参与血液凝固的重要部分,其水平低下可能导致或加重各种出血性疾病。正常人的Fib范围在3~4 g/L。但妊娠时,Fib浓度可上升至4~6 g/L。既往研究[13]发现,当孕妇的Fib>3 g/L,发生>2 500 mL的失血概率极低;但Fib水平 < 2.0 g/L时,进展为严重产后出血的阳性预测值高达100%,本研究结果与其基本相符。(6)产程与PPH密切相关,产程时长增加会对子宫平滑肌的兴奋收缩偶联效应产生影响,而长时间宫缩则会引起子宫平滑肌细胞胞膜上缩宫素受体数量减少[14-15],导致宫缩乏力和和不协调收缩,进行增加出血概率,第三产程时长是PPH的影响因素[16]。(7)胎盘粘连多因刮宫或宫腔感染引起,胎盘粘连常引起第三产程胎盘不完全剥离,致使产程时长增加,宫缩乏力,导致子宫血管不能及时的闭合,进而加大血液流失[17]。(8)胎儿体质量与PPH密切相关,胎儿过大会增加子宫肌纤维过度伸展而影响子宫收缩。而临床上常见胎儿较大的孕产妇在分娩过程出现产程延长、软产道裂伤、子宫收缩不协调等[18],这些表现因素均会增加PPH概率。因此,需对孕期胎儿体质量监测和孕妇相关营养指导,避免胎儿过度增长。
列线图模型作为在多因素回归分析基础上将多个预测指标整合后带有刻度的线段图形,表达简洁、易懂且自明性强,临床指导价值高。本研究根据孕妇自然分娩PPH的危险因素构建了列线图模型,经内部验证发现,列线图模型预测的灵敏度为0.819、特异度为0.715,说明列线图模型的判别能力较强。同时Bootstrap法自1 000次抽样对列线图模型的验证发现校准曲线的MAE为0.005,表明此列线图模型预测孕妇自然分娩PPH发生风险与实际发生具有良好的一致性。
综上所述,孕妇自然分娩PPH与年龄、多胎、妊高症、临产前D-二聚体、临产前Fib、第三产程时间、胎盘粘连及胎儿体质量相关。以此构建列线图预测模型,区分度良好。临床可依此筛选出可能发生PPH的孕妇,以便早期采取制定针对性预防措施,降低PPH风险。
孕妇自然分娩产后出血的风险列线图预测模型构建与验证
Construction and validation of a risk nomogram prediction model for postpartum hemorrhage in pregnant women during spontaneous delivery
-
摘要:
目的探讨孕妇自然分娩产后出血(PPH)的危险因素,并建立风险列线图预测模型。 方法收集在产科进行产检并最终阴道分娩的3 067例产妇的临床信息。以产妇分娩后24 h内是否发生PPH分为PPH组(n=229)和非PPH组(n=2 838)。对2组的临床信息进行比较,使用logistic回归分析筛选孕妇自然分娩PPH的危险因素并构建预测模型。用ROC曲线下面积(AUC)、灵敏度、特异度评价模型效能,用Bootstrap自抽样法对模型进行内部验证。 结果PPH组与非PPH组的年龄、多胎、妊娠期高血压疾病、临产前D-二聚体、临产前Fib、第三产程时间、胎盘粘连、胎儿体质量指标的比较差异均有统计学意义(P < 0.01)。多因素logistic回归分析显示,年龄高、多胎、有妊娠期高血压疾病、临产前D-二聚体升高、第三产程时间长、有胎盘粘连、胎儿体质量大均是孕妇自然分娩发生PPH的危险因素(P < 0.01),临产前Fib升高为孕妇自然分娩发生PPH的保护因素(P < 0.01)。利用上述8个指标构建列线图预测模型并验证,发现模型预测孕妇自然分娩PPH的AUC为0.824、灵敏度为0.819、特异度为0.715。经Bootstrap法自1 000次抽样对模型验证发现校准曲线的MAE为0.004,表明模型在预测孕妇自然分娩PPH发生风险与实际发生具有良好的一致性。 结论临床整合孕妇的年龄、胎数、妊娠期高血压疾病、临产前D-二聚体、临产前Fib、第三产程时间、胎盘粘连、胎儿体质量指标构建预测模型,可提高评估孕妇自然分娩PPH的准确性。 Abstract:ObjectiveTo explore the risk factors for postpartum hemorrhage (PPH) in pregnant women during spontaneous delivery, and to establish a risk nomogram prediction model. MethodsThe clinical information of 3 067 parturients who underwent an obstetric examination and eventually delivered vaginally in the department of obstetrics was collected.According to the occurence of PPH within 24 hours after delivery, the parturients were divided into PPH group (n=229) and non-PPH group (n=2 838).The clinical information of the two groups was compared, and logistic regression analysis was used to screen the risk factors for PPH in spontaneous delivery and a prediction model was established.The area under the ROC curve, sensitivity and specificity were used to evaluate the performance of the model, and Bootstrap self-sampling method was used to verify the model internally. ResultsThere were significant differences between PPH group and non-PPH group in age, multiple pregnancy, pregnancy induced hypertension, prenatal D-dimer, prenatal Fib, the third stage of labor, placental adhesion, and fetal body mass (P < 0.01).Multivariate logistic regression analysis showed that high age, multiple births, pregnancy induced hypertension, pre-partum D-dimer elevation, long third stage of labor, placenta adhesion, and large fetal body mass were all risk factors for PPH in spontaneous delivery of pregnant women (P < 0.01), and pre-partum Fib elevation was a protective factor for PPH in spontaneousl delivery of pregnant women (P < 0.01).By using the above 8 indicators to construct and verify the nomogram prediction model, it was found that the AUC of the model was 0.824, the sensitivity was 0.819, and the specificity was 0.715 for predicting PPH in spontaneous delivery of pregnant women.After 1 000 samples of Bootstrap method, the MAE of the calibration curve was 0.004, which showed that the model had a good consistency in predicting the risk of spontaneous delivery PPH in pregnant women and the actual occurrence. ConclusionsThe clinical integration of pregnant women's age, number of fetuses, pregnancy-induced hypertension, pre-partum D-dimer, pre-partum Fib, the third stage of labor, placental adhesions, and fetal weight indicators are used to construct a prediction model that can improve the accuracy of evaluating pregnant women's spontaneous delivery PPH. -
Key words:
- spontaneous childbirth /
- postpartum hemorrhage /
- risk factors /
- nomogram
-
表 1 2组的临床资料比较(x±s)
分组 n 年龄/岁 孕次 产次 孕周/周 多胎 剖宫产史 妊高症 妊娠期糖尿病 临产前Hb/(g/L) 临产前D-二聚体/(mg/L) PPH组 229 29.38±3.50 1.39±0.38 1.12±0.31 39.42±1.76 13 39 34 16 124.75±16.43 0.45±0.12 非PPH组 2 838 27.22±3.11 1.36±0.41 1.10±0.28 39.34±1.83 67 396 158 131 126.39±17.34 0.43±0.09 t — 10.01 1.07 1.03 0.64 6.53* 1.65* 31.10* 2.61* 1.38 3.14 P — < 0.01 >0.05 >0.05 >0.05 < 0.01 >0.05 < 0.01 >0.05 >0.05 < 0.01 分组 n 临产前PT/s 临产前APTT/s 临产前TT/s 临产前Fib/(g/L) 第一产程/min 第二产程/min 第三产程/min 胎盘粘连 胎儿体质量/kg PPH组 229 10.89±0.92 31.78±2.95 12.71±1.27 4.03±0.58 6 003.57±190.54 80.21±25.16 10.22±3.32 27 3.33±0.73 非PPH组 2 838 11.01±1.05 32.07±2.86 12.86±1.75 4.59±0.62 5 989.75±192.95 77.98±24.37 7.83±2.15 156 3.15±0.58 t — 1.68 1.47 1.27 13.21 1.04 1.33 15.41 14.96* 4.42 P — >0.05 >0.05 >0.05 < 0.01 >0.05 >0.05 < 0.01 < 0.01 < 0.01 *示χ2值  下载: 导出CSV
下载: 导出CSV
表 2 多因素logistic分析结果
变量 B SE Waldχ2 P OR(95%CI) 年龄 0.39 0.032 153.04 < 0.01 1.481(1.391~1.576) 多胎 1.76 0.414 18.12 < 0.01 5.825(2.588~13.114) 妊高症 1.07 0.251 18.26 < 0.01 2.927(1.788~4.790) 临产前D-二聚体 2.59 0.873 8.80 < 0.01 13.305(2.405~73.599) 临产前Fib -2.62 0.180 213.22 < 0.01 0.073(0.051~0.103) 第三产程时间 0.05 0.014 13.07 < 0.01 1.054(1.04~1.084) 胎盘粘连 0.77 0.271 8.06 < 0.01 2.155(1.268~3.662) 胎儿体质量 0.72 0.133 29.15 < 0.01 2.048(1.579~2.657)
下载: 导出CSV
-
[1] 刘兴会, 陈锰. 基于大数据的产后出血临床处理[J]. 中国实用妇科与产科杂志, 2018, 34(1): 33. [2] Prevention and management of postpartum haemorrhage: Green-top Guideline No.52[J]. BJOG, 2017, 124(5): e106. [3] 赵悦淑, 张龙梅, 王蕊, 等. 2005-2014年河南省孕产妇产科出血死亡原因及相关因素分析[J]. 中国妇幼保健, 2017, 32(7): 1357. [4] LEE HJ, LEE YJ, AHN EH, et al. Risk factors for massive postpartum bleeding in pregnancies in which incomplete placenta previa are located on the posterior uterine wall[J]. Obstet Gynecol Sci, 2017, 60(6): 520. doi: 10.5468/ogs.2017.60.6.520 [5] 谢幸, 苟文丽. 妇产科学[M]. 8版. 北京: 人民卫生出版社, 2013: 211. [6] EVENSEN A, ANDERSON JM, FONTAINE P. Postpartum hemorrhage: prevention and treatment[J]. Am Fam Physician, 2017, 95(7): 442. [7] VALDES V, ADONGO PB, NWAMEME AU, et al. Risk factors for self-reported postpartum hemorrhage in Ga East, Ghana[J]. Int J Gynaecol Obstet, 2018, 142(2): 201. doi: 10.1002/ijgo.12523 [8] 金洪运, 刘贵. 高龄孕妇剖宫产产后出血的影响因素分析[J]. 中国煤炭工业医学杂志, 2020, 23(3): 252. [9] BERNSTEIN PS, MARTIN JN, BARTON JR, et al. National partnership for maternal safety: consensus bundle on severe hypertension during pregnancy and the postpartum period[J]. Obstet Gynecol, 2017, 130(2): 347. doi: 10.1097/AOG.0000000000002115 [10] 张颖, 郝培培, 何佩. 高龄产妇产前血清FIB、D-二聚体、血红蛋白及血小板与产后出血的关系[J]. 中国妇幼保健, 2021, 36(5): 1021. [11] 李昀晖, 徐畅, 张文, 等. 妊娠晚期孕妇D-二聚体水平异常升高的因素分析[J]. 国际检验医学杂志, 2021, 42(1): 21. [12] 蒋一逍, 李力, 刘宿, 等. 纤维蛋白原在产后出血中的临床应用研究进展[J]. 解放军医学杂志, 2021, 46(5): 498. [13] KAVLE JA, STOLTZFUS RJ, WITTER F, et al. Association between anaemia during pregnancy and blood loss at and after delivery among women with vaginal births in Pemba Island, Zanzibar, Tanzania[J]. J Health Popul Nutr, 2008, 26(2): 232. [14] 韩宁玉, 王欣. 产程时限与产后出血相关性的临床研究[J]. 中华妇产科杂志, 2020, 55(10): 673. [15] MOLEIRO ML, GURDES-MARTINS L, MENDES A, et al. Modified pereira suture as an effective option to treat postpartum hemorrhage due to uterine atony[J]. Rev Bras Ginecol Obstet, 2018, 40(2): 92. [16] 倪胜莲, 曹琳琳, 郭志超, 等. 低风险初产妇产后出血风险预测[J]. 中国生育健康杂志, 2021, 32(2): 117. [17] 沈婕, 任青, 林元, 等. 二胎孕妇产后出血的危险因素及预测模型的建立[J]. 中国妇产科临床杂志, 2019, 20(5): 458. [18] 杨炜博, 唐仕芳, 马娟, 等. 美国妇产科医师协会"巨大儿指南(2020)"解读[J]. 中国计划生育和妇产科, 2020, 12(8): 15. -

 点击查看大图
点击查看大图
图(3)表(2)
计量
- 文章访问数: 1719
- HTML全文浏览量: 286
- PDF下载量: 7
- 被引次数: 0
