

-
ICU病人在治疗过程中极易出现一系列神经和精神心理性疾病综合征,如抑郁、焦虑、创伤后应激障碍等,其中危险程度较高的是谵妄[1]。谵妄是一种急性认知功能障碍,临床表现主要为急性意识波动和思维紊乱,常存在视幻觉、思维紊乱、定向力和记忆障碍等。有报道[2]显示,ICU病人谵妄发生率高达38%~87%。谵妄一旦发生,将严重影响疾病预后,治疗不及时会进一步加重认知功能障碍,导致机械通气时间延长、并发症和病死率增加,住院时间延长以及治疗费用增加[3]。目前对谵妄暂无有效的治疗方法,早期筛查和积极预防是改善谵妄预后的重要途径,病人进入ICU后即进行风险因素识别,对谵妄高风险人群实施干预,可降低谵妄的发病率、严重程度和谵妄持续时间。
通过构建ICU谵妄风险预测模型,一方面可有效帮助医护人员早期识别谵妄高风险人群,通过针对性预防措施减少谵妄的发生;另一方面也使病人清楚了解谵妄的发生风险,提高对谵妄危险因素防治的认知,增加治疗的依从性[4]。目前国内外构建ICU谵妄风险预测模型主要用于评估ICU病人入住24 h以后的谵妄发生风险[5],且多集中利用logistic回归模型进行谵妄预测模型的开发,忽略了模型的验证效能[6]。临床观察[7]发现,入住ICU<24 h的病人同样也是谵妄发生的高危人群,多达25%危重成人入住ICU<24 h内就会发生谵妄,其预防措施需要尽可能早地开始实施,因此,有必要纳入ICU<24 h的病人,不同模型对纳入的变量要求、进行模型建立过程中生成分支的算法也不同。基于此,本研究通过分析ICU<24 h的病人突发谵妄的主要危险因素,构建logistic回归模型和决策树模型,并进行前瞻性验证,以此为临床建立早期识别谵妄发生的防控机制。
-
选择2018年1月至2020年1月入我院ICU病人198例为模型组,根据24 h内谵妄诊断标准分为谵妄组88例和无谵妄组110例。
纳入标准:(1)年龄>18~80岁;(2)入住ICU24 h进行谵妄诊断;(3)符合临床研究的伦理学要求。排除标准:(1)入院前已经存在明显的神经或者精神性疾病;(2)入院前存在明显的意识障碍;(3)24 h内无法进行谵妄评估;(4)临床资料不完整。
-
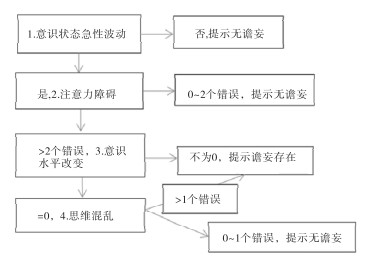
所有病人入院24 h内由责任医生和护士共同进行谵妄评估,采用ICU意识模糊评估法(CAM-ICU),具体流程见图 1。比较谵妄与无谵妄组病人的临床资料和生化指标,参照既往文献报道的主要危险因素,纳入性别、年龄、基础疾病类型、发病时间、急性生理与慢性健康(APACHE Ⅱ)评分、并发症、镇静时间、机械通气时间、氧合指数、血清神经烯醇化酶(NSE)和动脉血乳酸水平。通过单因素比较和多因素logistic回归分析筛选谵妄发生的独立危险因素。另选择2020年2月至2021年2月87例病人为验证组,受试者工作曲线(ROC)比较两种模型的预测效能。

图 1 CAM-ICU流程图
-
采用t检验、χ2检验、多因素logistic回归分析、决策树模型和ROC曲线。
-
与无谵妄病人相比,谵妄病人的年龄、APACHE Ⅱ评分和并发症增加、镇静时间和机械通气时间延长、血清NSE和动脉血乳酸升高,氧合指数降低,差异均有统计学意义(P<0.01)(见表 1)。
分组 n 男 女 年龄/岁 基础疾病类型 发病时间/h APACHE Ⅱ评分/分 外科手术 脑血管疾病 恶性肿瘤 心血管疾病 其他 无谵妄 110 59 51 60.7±5.3 27 35 20 22 6 6.4±2.3 26.7±5.9 谵妄 88 49 39 68.9±5.4 26 29 17 14 2 6.8±2.9 42.6±8.9 χ2 — 0.72 10.73* 2.18 1.08* 14.41* P — >0.05 <0.01 >0.05 >0.05 <0.01 分组 n 并发症 镇静时间/d 机械通气时间/d 氧合指数/mmHg 血清NSE/(ng/mL) 动脉血乳酸/(mmol/L) 颅脑严重水肿 重症感染 休克 多器官功能衰竭 无谵妄 110 5 4 3 3 3.7±0.9 2.9±0.6 402.6±56.9 36.5±8.7 1.6±0.4 谵妄 88 9 8 5 4 6.9±1.8 5.7±1.3 242.3±35.6 52.6±9.7 3.5±0.8 χ2 — 7.54 15.22* 18.68* 30.46* 15.32* 12.22* P — <0.01 <0.01 <0.01 <0.01 <0.01 <0.01 *示t值 表 1 谵妄的单因素分析
-
将病人的临床资料和生化指标作为自变量,谵妄作为因变量纳入多因素logistic回归分析显示,APACHE Ⅱ评分高、血清NSE和动脉血乳酸水平高是谵妄发生的独立危险因素(P<0.01)(见表 2)。根据筛选独立危险因素的权重进行定量赋值,建立logistic回归模型=-0.232+0.564×(APACHE Ⅱ评分)+0.446×(血清NSE)+0.402×(动脉血乳酸)。
因素 B Waldχ2 P OR OR95%CI 评分 APACHE II评分 0.564 6.23 <0.01 1.659 1.325~1.958 3 血清NSE 0.446 5.96 <0.01 1.524 1.231~1.895 2 动脉血乳酸 0.402 5.53 <0.01 1.428 1.124~1.785 2 常数项 -0.232 — — — — — 表 2 谵妄的多因素分析
-
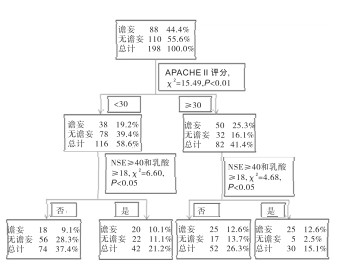
根据筛选独立危险因素建立决策树模型见图 2。

图 2 谵妄发生的决策树预测模型
-
验证组ROC分析显示,决策树模型的AUC值高于logistic回归模型,差异有统计学意义(P<0.01)(见表 3)。
模型 AUC 95%CI P logistic回归模型 0.812 0.756~0.895 <0.01 决策树模型 0.865 0.805~0.915 <0.01 决策树模型VSlogistic回归模型 0.053 0.023~0.088 <0.01 表 3 谵妄模型的预测效能比较
-
风险预测模型是以疾病的多病因为基础建立统计学模型,预测某些特征人群未来某种疾病发生的概率。logistic回归是临床应用最广泛的一种统计模型,缺点是对非线性、具有交互作用的数据处理效能较低,且不能直观显示各个变量在所预测结果中的重要性[8]。决策树作为一种非参数统计方法,在克服数据共线性问题的同时,可以根据可用数据构建预测模型,结果显示为树状结构图,还可以对纳入指标的重要性进行排序,确定主要的预测因子,便于评分系统的构建[9-10],因此,构建预测ICU病人早期谵妄的决策树模型,形成相应的决策树评分系统并进行前瞻性验证显得尤为重要。
ICU病人往往病情急、重,变化快,并发症多,预后较差。机体在遭受内外环境应激情况下易诱发谵妄等神经精神性疾病,同时谵妄也是神经不可逆性损伤的前兆,对提示疾病进展、预后不良具有十分重要的临床意义,需要引起医护人群及时识别谵妄的发生以及预测谵妄高危人群,及时给予恰当的干预措施,以预防或者降低谵妄的发生风险[11]。根据CAM-ICU能够在病人入院后24 h内、24 h后、转出ICU至普通病房以及出院前等多个时间点进行定量评估[12],但是不能指导临床医护人群早期识别谵妄的高危病人,因此,需要利用临床最易获得的资料筛选可能诱发谵妄发生的高危因素,并建立定量预测模型以指导临床实践。
本研究显示,谵妄病人的年龄、APACHE Ⅱ评分和并发症增加、镇静时间和机械通气时间延长、血清NSE和动脉血乳酸升高,氧合指数降低。本研究是在参考既往文献报道的主要高危因素的基础上进行筛选,发现高龄病人谵妄的发生率明显增加,与既往研究[13]结果一致。高龄病人对应激代偿机制下降,同时多合并基础疾病,对机械通气和镇静管理的耐受性较差,内源性有害因子易蓄积,都是导致谵妄发生的不利原因[14]。APACHE Ⅱ评分是目前临床评估危重症病人病情变化以及预后的主要客观工具,具有较好的准确性[15]。该研究的决策树模型也将其作为第一层筛选依据,且具有较高的权重比。ICU病人普遍需要接受镇静和机械通气管理,对辅助病人渡过疾病高危期具有十分重要的意义。但同时,镇静和机械通气管理不当或者应用时间过长,也易增加呼吸机相关肺炎、低血压、呼吸或者循环抑制等并发症,需要加强巡视,预防镇静和机械通气管理期间的并发症发生[16-17]。NSE是中枢神经系统分泌和表达的一类重要神经递质,对提示神经系统损伤具有较好的敏感性和准确性[18]。有研究证实[19],NSE与多种脑源性疾病继发的认知功能障碍有紧密联系,是认知功能损伤的早期敏感性生物标志物。乳酸和氧合指数是动脉血气分析的重要指标,对提示低氧或者二氧化碳蓄积有较好的准确性,也是谵妄等多种缺氧诱导疾病的客观量化指标[20]。
该研究通过logistic回归分析显示,APACHE Ⅱ评分、血清NSE和动脉血乳酸水平是谵妄发生的独立危险因素。分别构建logistic回归模型和决策树模型,经验证组ROC分析显示,决策树模型的AUC值高于logistic回归模型。提示决策树模型比传统logistic回归模型在预测ICU谵妄发生风险方面可能具有更高的效能,更有利于指导临床医护人员的应用。该研究的创新点是比较了2种模型在预测ICU谵妄发生风险方面的应用潜力,同时利用外部前瞻性队列数据进行验证,可信度更高。
本研究为今后ICU工作人员在病人24 h内准确识别和筛选谵妄高风险人群提供了更加直观、更加高效的决策树预测模型,并依次建立最佳的防控机制。在积极治疗原发疾病的同时,预防谵妄的发生,定期进行APACHE Ⅱ评分、血清NSE和动脉血乳酸检测,与疾病治疗进程进行比对,对异常结果需要高度重视。对筛选出的谵妄高风险人群进行重点关注,努力寻找诱发谵妄发生的高危因素进行干预。
综上所述,ICU病人24 h内突发谵妄的发生率较高,多个危险因素可能参与了谵妄的发生,包括APACHE Ⅱ评分、血清NSE和动脉血乳酸水平升高,通过构建决策树模型比传统logistic回归模型可能具有更高的预测效能,为指导临床医护人员早期正确识别谵妄高风险群体提供了更佳的评估手段。
ICU病人突发谵妄的防控机制研究
Study on the best prevention mechanism for sudden delirium in ICU patients
-
摘要:
目的分析ICU病人突发谵妄的主要危险因素,构建logistic回归模型和决策树模型,并进行前瞻性验证,为临床建立早期识别谵妄发生的最佳防控机制。 方法随机选取2018年1月至2020年1月病人198例为模型组,开展回顾性分析,根据24 h内谵妄诊断标准分为谵妄88例和无谵妄110例,多因素logistic回归分析筛选危险因素。另选择2020年2月至2021年2月87例病人为验证组,受试者工作特征曲线(ROC)比较2种模型的预测效能。 结果与无谵妄病人相比,谵妄病人的年龄、急性生理与慢性健康(APACHE Ⅱ)评分和并发症增加, 镇静时间和机械通气时间延长, 血清神经烯醇化酶(NSE)和动脉血乳酸升高,氧合指数降低(P < 0.01)。logistic回归分析显示,APACHE Ⅱ评分高、血清NSE和动脉血乳酸水平高是谵妄发生的独立危险因素(P < 0.01)。分别构建logistic回归模型和决策树模型,经验证组ROC分析显示,决策树模型的曲线下面积0.865高于logistic回归模型的0.812(P < 0.01)。 结论ICU病人24 h内突发谵妄的发生率较高,多个危险因素可能参与了谵妄的发生,包括APACHE Ⅱ评分、血清NSE和动脉血乳酸水平升高,决策树模型比传统logistic回归模型可能具有更高的预测效能,可为指导临床医护人员早期正确识别谵妄高风险群体提供了更佳的评估手段。 Abstract:ObjectiveTo analyze the main risk factors of sudden delirium in ICU patients, construct logistic regression model and decision-tree model through a prospective verification to establish the best prevention mechanism for early identification of delirium. MethodsA total of 198 ICU patients from January 2018 to January 2020 were retrospectively summarized as the model group.According to the diagnostic criteria of delirium within 24 hours, they were divided into delirium group (n=88) and non-delirium group (n=110).The risk factors were screened by multivariate logistic regression analysis.In addition, 87 patients from February 2020 to February 2021 were choosed as the validation group.Receiver operating characteristic curve was used to compare the predictive efficacy of the two models. ResultsCompared with the patients without delirium, the age, acute physiology and chronic health (APACHE Ⅱ) score and complications of the patients with delirium were increased, sedation time and mechanical ventilation time were prolonged, serum neuro-specific enolase(NSE) and arterial blood lactic acid were increased, and oxygenation index was decreased (P < 0.01).Logistic regression analysis showed that APACHE Ⅱ score, serum NSE and arterial blood lactate level were independent risk factors for delirium (P < 0.01).The area under the curve of the decision-tree model was higher than that of logistic regression model (P < 0.01). ConclusionsThe incidence of sudden delirium within 24 hours in ICU patients is high, and multiple risk factors may be involved in the occurrence of delirium, including APACHE Ⅱ score, serum NSE and arterial blood lactic acid level.The decision-tree model may have a higher predictive efficacy than traditional logistic regression model, which provides a better evaluation method for guiding clinical medical staff to correctly identify high-risk groups of delirium in early stage. -
Key words:
- delirium /
- decision-tree model /
- neuro-specific enolase
-
表 1 谵妄的单因素分析
分组 n 男 女 年龄/岁 基础疾病类型 发病时间/h APACHE Ⅱ评分/分 外科手术 脑血管疾病 恶性肿瘤 心血管疾病 其他 无谵妄 110 59 51 60.7±5.3 27 35 20 22 6 6.4±2.3 26.7±5.9 谵妄 88 49 39 68.9±5.4 26 29 17 14 2 6.8±2.9 42.6±8.9 χ2 — 0.72 10.73* 2.18 1.08* 14.41* P — >0.05 <0.01 >0.05 >0.05 <0.01 分组 n 并发症 镇静时间/d 机械通气时间/d 氧合指数/mmHg 血清NSE/(ng/mL) 动脉血乳酸/(mmol/L) 颅脑严重水肿 重症感染 休克 多器官功能衰竭 无谵妄 110 5 4 3 3 3.7±0.9 2.9±0.6 402.6±56.9 36.5±8.7 1.6±0.4 谵妄 88 9 8 5 4 6.9±1.8 5.7±1.3 242.3±35.6 52.6±9.7 3.5±0.8 χ2 — 7.54 15.22* 18.68* 30.46* 15.32* 12.22* P — <0.01 <0.01 <0.01 <0.01 <0.01 <0.01 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 谵妄的多因素分析
因素 B Waldχ2 P OR OR95%CI 评分 APACHE II评分 0.564 6.23 <0.01 1.659 1.325~1.958 3 血清NSE 0.446 5.96 <0.01 1.524 1.231~1.895 2 动脉血乳酸 0.402 5.53 <0.01 1.428 1.124~1.785 2 常数项 -0.232 — — — — —
下载: 导出CSV
表 3 谵妄模型的预测效能比较
模型 AUC 95%CI P logistic回归模型 0.812 0.756~0.895 <0.01 决策树模型 0.865 0.805~0.915 <0.01 决策树模型VSlogistic回归模型 0.053 0.023~0.088 <0.01
下载: 导出CSV
-
[1] KOTFIS K, MARRA A, ELY EW. ICU delirium-a diagnostic and therapeutic challenge in the intensive care unit[J]. Anaesthesiol Intensive Ther, 2018, 50(2): 160. doi: 10.5603/AIT.a2018.0011 [2] 赵洁, 蒋月娟. ICU老年高血压脑出血病人谵妄发生状况及其影响因素分析[J]. 全科护理, 2021, 19(9): 1283. [3] 张玉宝, 王汇, 程岚. COPD机械通气病人谵妄发生风险的列线图预测模型构建与评估[J]. 蚌埠医学院学报, 2021, 46(11): 1611. doi: 10.13898/j.cnki.issn.1000-2200.2021.11.029 [4] 韩汝宁, 陈春丽, 彭雅琴. eCASH理念结合早期分级康复训练在ICU机械通气病人中的应用研究[J]. 蚌埠医学院学报, 2021, 46(9): 1280. doi: 10.13898/j.cnki.issn.1000-2200.2021.09.034 [5] 王永华, 李小会, 陈艳蓉. 重症监护室老年脑损伤机械通气病人发生谵妄的危险因素分析[J]. 全科护理, 2020, 18(36): 5146. doi: 10.12104/j.issn.1674-4748.2020.36.036 [6] 隋伟静, 宫晓艳, 庄一渝. ICU谵妄风险预测模型的研究进展及趋势分析[J]. 护士进修杂志, 2020, 35(22): 2054. [7] FLANNERY AH, OYLER DR, WEINHOUSE GL. The impact of interventions to improve sleep on delirium in the ICU: a systematic review and research framework[J]. Crit Care Med, 2016, 44(12): 2231. doi: 10.1097/CCM.0000000000001952 [8] 黎春艳, 黄秀芳, 黄幼平. 谵妄评估约束分级式护理在重症监护室病人护理中的应用研究[J]. 全科护理, 2020, 18(36): 5100. doi: 10.12104/j.issn.1674-4748.2020.36.021 [9] 丁工物, 刘树娟, 李晋磊. 利用决策树和随机森林评估社区老人生活方式风险因素对认知障碍的影响[J]. 中华疾病控制杂志, 2020, 24(4): 485. [10] 王潇, 郭宗君, 张文青. 血管性认知功能障碍高危因素的决策树模型研究[J]. 中华行为医学与脑科学杂志, 2017, 26(6): 534. doi: 10.3760/cma.j.issn.1674-6554.2017.06.011 [11] BLAIR GJ, MEHMOOD T, RUDNICK M. Nonpharmacologic and medication minimization strategies for the prevention and treatment of ICU delirium: a narrative review[J]. J Intensive Care Med, 2019, 34(3): 183. doi: 10.1177/0885066618771528 [12] 冯雅笛, 杨芳宇, 李京连. 智能版与纸版CAM-ICU谵妄评估的一致性研究[J]. 护理研究, 2021, 35(1): 15. [13] KANOVA M, SKLIENKA P, ROMAN K. Incidence and risk factors for delirium development in ICU patients—a prospective observational study[J]. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub, 2017, 161(2): 187. doi: 10.5507/bp.2017.004 [14] 王华英, 由春梅, 谢涛. 术后谵妄患者的临床特点及危险因素[J]. 中国老年学杂志, 2019, 39(22): 5538. doi: 10.3969/j.issn.1005-9202.2019.22.046 [15] 聂晓莉, 薛旗山, 赵秋红. APACHEⅡ评分对重症肺部感染机械通气患者谵妄预测价值研究[J]. 创伤与急危重病医学, 2019, 7(1): 31. [16] 金玲丽, 袁莉萍, 江海娇. 镇静镇痛集束护理对ICU病人谵妄影响的Meta分析[J]. 循证护理, 2020, 6(8): 762. [17] MALDONADO JR. Acute brain failure: pathophysiology, diagnosis, management, and sequelae of delirium[J]. Crit Care Clin, 2017, 33(3): 461. doi: 10.1016/j.ccc.2017.03.013 [18] 王舰, 邬晓臣, 刘敬臻. 神经损伤标志物与老年患者心脏瓣膜置换术后谵妄的相关性[J]. 中华老年多器官疾病杂志, 2020, 19(12): 886. [19] 惠姣洁, 严正, 梁锋鸣. 血浆BDNF、NSE和S100β的动态变化与ICU患者谵妄的关系[J]. 中华急诊医学杂志, 2018, 27(10): 1132. doi: 10.3760/cma.j.issn.1671-0282.2018.10.014 [20] 李洁, 李芬, 邢柏. 早期动脉血乳酸与乳酸清除率对老年脓毒性休克患者谵妄发生的预测价值[J]. 重庆医学, 2021, 4(1): 1. doi: 10.3969/j.issn.1671-8348.2021.01.001 -

 点击查看大图
点击查看大图
图(2)表(3)
计量
- 文章访问数: 3816
- HTML全文浏览量: 300
- PDF下载量: 1
- 被引次数: 0
