



-
三角韧带属踝关节内侧最坚强的结构,可以保障距骨在踝穴中解剖位置的正常,避免发生外移或外旋[1-2]。此外,三角韧带还对足踝部负重与正常运动功能存在重要影响。若三角韧带损伤延误治疗,易引发韧带松弛、复位不良,进而导致踝部慢性疼痛、踝关节不稳定以及创伤性关节炎等一系列问题[3]。在踝关节损伤中,约13%的病人合并有三角韧带损伤[1],但关于其处理方案目前尚有争议。部分学者认为,若踝关节通过切开内固定手术后复位、愈合良好,三角韧带可通过瘢痕组织修复愈合;但亦有部分研究[4-5]指出,若三角韧带断裂后未能尽早修复,可造成病人行走不稳、足外翻或踝关节疼痛等后遗症。为此,本研究回顾性分析踝关节骨折合并三角韧带断裂病人72例资料,以探讨带线锚钉修复三角韧带断裂在切开复位内固定手术中的临床价值。现作报道。
HTML
-
72例均为我科2013年9月至2016年9月收治的踝关节骨折并三角韧带断裂病人,均接受切开复位内固定手术治疗,依据术中对三角韧带的处理方式不同分为观察组36例,术中联合带线锚钉进行三角韧带修复处理;对照组36例,术中不予以三角韧带修复。2组病人性别、年龄、受伤时间、骨折部位和骨折分型、致伤原因等基线资料差异均无统计学意义(P>0.05)(见表 1),具有可比性。
分组 n 男 女 年龄/岁 受伤时间/d 骨折部位 Lauge-Hansen分型 致伤原因 左踝 右踝 旋后外旋型 旋前外旋型 旋前外展型 坠落伤 车祸伤 扭伤 观察组 36 21 15 45.6±6.4 4.3±1.3 16 20 7 19 10 12 15 9 对照组 36 23 13 46.2±5.8 4.2±1.5 17 19 8 20 8 11 15 10 χ2 — 0.23 0.42* 0.30* 0.06 0.32 0.10 P — >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 *示t值 -
纳入标准:(1)经影像学检查结合临床症状,诊断为踝关节骨折并三角韧带断裂,且伴有下胫腓联合损伤者;(2)接受踝关节骨折的切开复位内固定手术者。排除标准:(1)未伴有三角韧带完全断裂;(2)陈旧性三角韧带断裂;(3)采用保守治疗者;(4)临床资料或随访资料不全者。
-
2组均由同一组医生完成手术。均先采用支具进行临时固定,对伤处进行冰敷,给予甘露醇静脉滴注以消肿。均于伤后2~8 d进行手术,患足皮肤出现褶皱则为手术最佳时间。对伴有高血压、糖尿病的病人,需控制血压、血糖水平在正常范围后再进行手术。
-
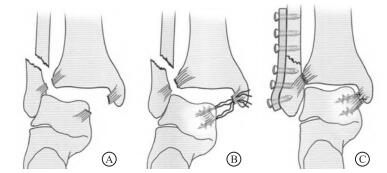
观察组:给予常规硬膜外麻醉,并保持仰卧位,在伤肢大腿上采用止血带。首先在踝内侧作弧形切口,逐层分离,暴露出三角韧带浅层,可见三角韧带浅层断裂,但断裂部位存在差异(其中6例断裂于距骨止点处,19例体部断裂,11例内踝前丘起点处撕脱),其断端为马尾状,且部分卷进关节间隙。外翻踝关节以彻底清理关节内血肿,将嵌入软组织拨开,并将嵌入关节间隙内的韧带松解,纠正韧带扭转。必要时还可将胫后肌腱鞘切开,向后方牵拉肌腱,探查三角韧带深层(其深层断裂部位有差异,其中21例为距骨内侧面止点撕裂,10例为中部撕裂,另5例为内踝后丘与丘间沟部撕裂)。针对三角韧带深、浅层的撕裂部位,在内踝或距骨处拧入带线锚钉2枚(直径5.0 mm,美国Johnson公司),经尾部预置缝线编织缝合断端,重建止点,但无需将缝线打结。调节手术床向健侧倾斜,并于患侧臀下垫一软垫,便于外踝、后踝操作。在腓骨后外侧作切口,显露出外踝骨折,解剖复位后采用锁定钢板螺钉固定。针对后踝骨折块较大病人,复位后行空心加压螺钉固定。术中通过腓骨牵拉试验,4例为阳性者,其中2例Maisonnuve骨折,经2枚直径4.0 mm螺钉内固定下胫腓;2例旋前外展型骨折,经1枚螺钉内固定下胫腓。螺钉置入方向即由后向前30°左右,从腓骨到胫骨前内横穿固定3层皮质,在踝关节中立位拧进。腓骨牵拉试验阴性者,未对下胫腓进行固定。固定完毕后,采用C型臂X线机透视检查内踝、外踝以及下胫腓联合复位情况,确认内固定可靠,复位良好。最后对踝关节适当内翻,对三角韧带锚钉缝线拉紧打结(见图 1)。松开止血带,若术后渗血严重则放置皮下引流,严密缝合皮下关闭切口,适当包扎手术切口。对照组:病人麻醉方式、踝关节骨折的切开复位内固定方式均与观察组一致,但术中不予三角韧带缝合处理。

-
2组均于术后2~3 d切口换药,严密观察切口愈合情况,若放置引流则需24 h内拔出。对照组术后予以塑形支具将患肢固定,禁止膝、踝关节运动,以免影响三角韧带的粘连愈合过程;术后8周可去除支具进行踝关节伸屈锻炼。观察组术后3 d可指导进行足趾与踝关节功能锻炼。未放置下胫腓螺钉者,术后6周可进行部分负重,12周后可完全负重;放置下胫腓螺钉病人术后12周取出螺钉后可负重行走。
-
(1) 术后1年内进行随访,经踝关节正侧位X线片观察骨折愈合情况、踝穴内侧距离和踝关节跖屈、背伸范围。(2)进行AOFAS踝-后足功能评分[6],分数为0~100分,其中90~100分为优;75~89分为良;50~74分为可,< 50分为差。
-
采用t检验和χ2检验。
1.1. 一般资料
1.2. 选择标准
1.3. 手术方法
1.3.1. 术前准备
1.3.2. 手术处理
1.3.3. 术后处理
1.4. 效果评定
1.5. 统计学方法
-
全部病人均手术顺利,骨折复位良好;术后均获随访6~16个月。2组病人骨折愈合时间为8~12周,均未发生骨折愈合延迟、感染、骨髓炎等并发症。截至末次随访时,观察组的踝穴内侧距离为(3.92±1.76)mm,低于对照组的(4.85±2.03)mm(t=2.08,P < 0.05)(见图 2)。对照组术后有6例发生踝关节内侧不稳现象,予以延长支具固定时间,症状有所改善;3例踝关节的跖屈活动明显受限;观察组无一例发生踝关节内侧不稳和螺钉脱出等并发症。

-
截至末次随访时,观察组的踝关节跖屈和背伸活动度均优于对照组(P < 0.01)(见表 2)。
分组 n 踝关节跖屈/(°) 踝关节背伸/(°) 观察组 36 17.02±4.26 34.59±6.41 对照组 36 13.34±5.18 29.33±4.07 t — 3.29 4.16 P — < 0.01 < 0.01 -
末次随访时,2组踝关节功能均得到良好恢复,AOFAS踝-后足功能评分观察组(88.31±5.62)分,对照组(79.26±7.75)分,观察组评分高于对照组(t=5.67, P < 0.01)。观察组总优良率为86.1%,对照组为75.0%,差异无统计学意义(P>0.05)(见表 3)。
分组 n 优 良 可 差 优良率/% χ2 P 观察组 36 17 14 4 1 86.1 1.42 >0.05 对照组 36 12 14 6 3 75.0 合计 72 29 28 10 4 79.2
2.1. 骨折复位和并发症情况

2.2. 踝关节活动度比较
2.3. 功能恢复情况
-
三角韧带作为胫骨远端与距骨的连接组织,具有维持内踝稳定性的作用。踝关节处于中立位,跖屈位或背伸位时,三角韧带均呈紧张状态。临床一致认为,三角韧带深层对踝关节稳定作用最为显著,其能够通过控制距骨过度旋前从而保障关节稳定,三角韧带浅层仅能够防止距骨过度外展倾斜[7],但关于其处理方案目前尚有争议。既往认为,若踝关节骨折经切开复位满意,三角韧带可通过瘢痕形成过程自行修复,无需手术缝合;但近来有不少学者指出,若三角韧带断裂未予处理,可导致内踝稳定性受明显影响,甚至出现后足外翻、行走不稳及踝内侧痛等明显症状[8-9]。本研究的对照组36例均未予以三角韧带缝合处理,随访期间发生6例踝关节内侧不稳、3例踝关节跖屈活动明显受限,亦证实了这一点。全部病人均手术顺利,骨折复位良好;术后均获随访6~16个月。2组病人骨折愈合时间为8~12周,均未发生骨折愈合延迟、感染、骨髓炎等并发症。截至末次随访时,观察组的踝穴内侧距离低于对照组,但本研究中2组优良率差异无统计学意义,需要进一步扩大样本进行验证。同时,观察组的踝关节跖屈和背伸活动度均优于对照组,均证实了三角韧带行带线锚钉修复的必要性,与高武长等[4-5]研究结果一致。
本研究观察组36例病人,均在切开复位内固定的同时,采用带线锚钉重建三角韧带止点并对三角韧带解剖修复。根据锚钉的支持原理,在内踝或距骨韧带止点固定三角韧带断端。该方式优势在于:(1)方式简单灵活,便于对置入位置进行灵活调整,韧带可经尾端缝线缝合,能够进行多点固定,提高了稳定性;(2)锚钉在埋入骨内之后,双加压固定更为牢固稳定,便于早期功能锻炼;(3)无需再次手术将锚钉取出,可减少病人二次手术的痛苦,减轻其医疗负担[10]。但带线锚钉的手术中需注意:(1)首先在踝关节内侧做切口,将内踝间隙清理干净,对三角韧带进行探查,在韧带断裂处置入锚钉,采用锚钉尾线将三角韧带缝合,但不收紧打结,在后踝、腓骨内固定后内翻踝关节再收紧、打结缝线。(2)术中需注意锚钉放置的角度与位置,以防移位松动,或脱出进入关节腔[11]。(3)若局部骨质伴有骨质疏松或者存在囊性变,应禁用锚钉固定[12]。
综上所述,针对踝关节骨折并三角韧带断裂应用带线锚定修复,能够促进踝穴、踝关节结构恢复,有助于恢复踝关节跖屈和背伸活动度,增强踝关节稳定性,临床效果满意。本研究的不足之处在于仅作回顾性分组对照研究,且样本数较少,尚有待大样本、多中心前瞻性研究进一步论证。
 DownLoad:
DownLoad: