




-
胫骨中下段骨折属常见四肢创伤骨折,占全身骨折3%~10%,常因高处坠落、交通事故等高能量暴力导致,降低病人日常生活能力与生活质量[1-3]。内固定手术为治疗胫骨中下段骨折的重要手段,但因胫骨中下段皮下组织覆盖较少,血供不丰富,术后易出现骨折不愈合或延迟、畸形愈合等并发症[4-5]。如何于符合力学固定条件下尽可能保护骨折端血供,加速骨折愈合一直为临床治疗的重点、难点。闭合复位交锁髓内钉内固定(IMN)、切开复位有限接触钢板内固定均为治疗胫骨中下段骨折的重要术式,但目前关于2种术式应用于胫骨中下段骨折的优劣情况尚存在一定争议。本研究旨在观察两者治疗胫骨中下段骨折的效果,并首次分析对病人炎症应激、血清碱性磷酸酶(ALP)、骨钙素N端中分子片段(N-MID)、Ⅰ型胶原羧基末端肽片段(β-CTX)表达的作用,以期为临床治疗提供一定支持。现作报道。
HTML
-
选取2017-2019年我院收治胫骨中下段骨折病人80例,按随机数字表分为IMN组和对照组,各40例。2组性别、年龄、体质量指数(BMI)、病程、骨折原因、骨折AO分型、骨折部位等一般资料差异无统计学意义(P>0.05)(见表 1),均具有可比性。本研究经医院伦理委员会同意。
分组 n 男 女 年龄(x±s)/岁 BMI(x±s)/(kg/m2) 病程(x±s)/d 骨折原因 骨折AO分型 骨折部位 重物砸伤 跌倒摔伤 高处坠落伤 交通事故伤 C型 B型 A型 左侧 右侧 IMN组 40 23 17 43.18±9.41 21.92±1.63 2.42±0.39 7 10 5 18 6 12 22 17 23 对照组 40 26 14 45.06±8.93 22.08±1.57 2.51±0.43 6 9 4 21 8 14 18 22 18 χ2 — 0.47 0.92* 0.45* 0.98* 0.47 0.84 1.25 P — >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 >0.05 *示t值 -
(1) 经X线片确诊为胫骨中下段骨折;(2)新鲜、闭合性、单侧骨折;(3)受伤原因明确,有明确手术适应证;(4)入组前未采取有关治疗;(5)受伤前患肢功能良好;(6)知晓本研究,签订知情同意书。
-
(1) 患肢存在筋膜间室综合征、血管神经损伤等严重创伤有关并发症;(2)病理性、陈旧性骨折;(3)骨折线涉及踝关节面或极远端;(4)合并严重骨质疏松;(5)合并严重高血压、糖尿病;(6)合并凝血功能障碍、精神系统疾病、恶性肿瘤;(7)合并心、肺、肝、肾等脏器功能严重障碍。
-
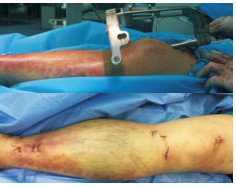
对照组:行切开复位有限接触钢板内固定:病人腰麻或全身麻醉,平卧位,患侧大腿根部绑充气止血带;于小腿内踝处纵行切口约9 cm,逐层切开皮肤与皮下组织,顺胫骨内侧面潜行分离形成通道,直视或闭合下对骨折行解剖复位;克氏针临时固定后,顺通道插入合适规格钢板,塑形后放置恰当,戳孔后置入螺钉,确保骨折两端各有6个有效皮质固定(见图 1)。

IMN组:麻醉、体位选取与对照组一致,患侧大腿根部绑充气止血带,胫骨髓内钉固定系统购于大博公司;髌下入路需屈膝90°~120°,屈髋60°~90°,行膝正中偏内侧入路,切口长4~5 cm,沿着髌韧带内侧逐渐进入,在必要时可将部分髌韧带纵行切开,充分暴露胫骨平台斜坡,在斜坡顶点偏内侧开口,置入导针。髌上入路膝关节屈曲15°,于髌上2 cm处作3 cm纵行切口,分离股直肌后进入髌上囊,将专用保护套穿髌股关节间隙到达胫骨平台前方。于透视下确保导针位置居中,缓缓牵引下肢,实施复位、维持力线,在测深后扩髓到出现明显阻力,沿着导针指引方向置入规格适合髓内钉,于透视下调节肢体长度与旋转,骨折断端复位效果满意后,安置锁定钉对准导航装置,置远近端锁钉(见图 2)。

2组术后均抬高患肢并采取消肿处理,预防性予以抗生素1~2 d,鼓励病人采取早期膝踝关节功能、肌肉收缩锻炼,并依据恢复与骨折愈合情况逐渐采取部分负重与负重行走。
-
(1) 炎症应激指标检测:分别于术前、术后1 d、术后3 d抽取病人清晨空腹肘静脉血样5 mL,应用离心机离心10 min,转速3 000 r/min,采集上层血清,以酶联免疫吸附法测定血清肿瘤坏死因子-α(TNF-α)、白细胞介素-8(IL-8)、白细胞介素-6(IL-6)、去甲肾上腺素(NE)、血管紧张素-Ⅱ(Ang-Ⅱ)、皮质醇(Cor)水平,试剂盒购于上海酶联生物科技有限公司;(2)骨代谢指标检测:分别于术前、术后1周及1个月抽取病人清晨空腹肘静脉血样3 mL,离心方法同上,取上层血清,以放射免疫法测定血清ALP、β-CTX水平,双抗体夹心酶联免疫吸附法测定N-MID水平,试剂盒购于深圳晶美生物工程有限公司,有关操作严格按试剂盒说明书进行。
-
(1) 手术情况。(2)并发症。(3)术前、术后1 d、术后3 d血清炎症反应指标(TNF-α、IL-8、IL-6)水平。(4)术前、术后1 d、术后3 d血清应激反应指标(NE、Ang-Ⅱ、Cor)水平。(5)术前、术后1周及1个月血清ALP、N-MID、β-CTX水平。(6)术后应用电话随访或门诊复查等形式随访6个月,应用Johner-Wruhs评分系统评价病人踝关节功能恢复情况,满分0~100分,分为差(评分≤70分)、可(评分处于71~80分)、良(评分处于81~90分)、优(评分>90分)4个等级,踝关节功能恢复优良率=(良+优)/总例数×100%[6];以美国膝关节协会评分(AKSS)评价膝关节功能,满分200分,分为差(评分 < 120分)、可(评分120~ < 140分)、良(评分140~ < 170分)、优(评分≥170分)4个等级,膝关节功能恢复优良率=(良+优)/总例数×100%[7]。
-
采用独立样本t检验和χ2检验。
1.1. 一般资料
1.2. 病例选择标准
1.2.1. 纳入标准
1.2.2. 排除标准
1.3. 方法
1.4. 检测方法
1.5. 观察指标
1.6. 统计学方法
-
2组手术时间比较差异无统计学意义(P>0.05);IMN组切口长度、术后下地时间、骨折愈合时间短于对照组,术中出血量、术后引流量、术后24 h患侧小腿中段周径/术前周径比值均低于对照组(P < 0.01)(见表 2)。
分组 n 手术时间/min 切口长度/cm 术后下地时间/周 骨折愈合时间/周 术中出血量/mL 术后引流量/mL 术后24 h患侧小腿中段周径/术前周径比值 IMN组 40 104.75±15.48 4.19±0.35 9.27±2.35 19.58±4.74 74.12±9.50 58.47±7.36 1.19±0.34 对照组 40 102.64±17.29 9.86±1.24 12.18±2.60 28.37±7.08 187.53±37.61 139.51±18.72 1.57±0.41 t — 0.58 27.83 5.25 6.52 18.49 25.48 4.51 P — >0.05 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 -
IMN组并发症发生率低于对照组(P < 0.05)(见表 3)。
分组 n 延迟愈合或不愈合 感染 膝关节疼痛 切口皮缘坏死 总发生 χ2 P IMN组 40 1(2.50) 0(0.00) 1(2.50) 0(0.00) 2(5.00) 对照组 40 3(7.50) 2(5.00) 3(7.50) 1(2.50) 9(22.50) 5.17 < 0.05 合计 80 4(5.00) 2(2.50) 4(5.00) 1(1.25) 11(13.75) -
2组术前血清TNF-α、IL-8、IL-6水平比较差异无统计学意义(P>0.05);2组术后1 d、3 d血清TNF-α、IL-8、IL-6水平均较术前增高(P < 0.01),但IMN组均低于对照组(P < 0.01)(见表 4)。
分组 n 术前 术后1 d 术后3 d F P MS组内 TNF-α/(ng/mL) IMN组 40 1.46±0.19 2.04±0.28** 2.27±0.34** 90.87 < 0.01 0.077 对照组 40 1.39±0.23 3.25±0.37** 3.48±0.41** 440.38 < 0.01 0.119 t — 1.48 16.49 14.37 — — — P — >0.05 < 0.01 < 0.01 — — — IL-8/(pg/mL) IMN组 40 8.74±1.61 11.60±2.06** 12.85±2.71** 37.57 < 0.01 4.727 对照组 40 9.12±1.49 14.07±2.63** 16.96±3.47** 80.07 < 0.01 7.059 t — 1.10 4.68 5.90 — — — P — >0.05 < 0.01 < 0.01 — — — IL-6/(pg/mL) IMN组 40 8.83±1.40 10.47±1.61** 11.93±1.85** 36.19 < 0.01 2.658 对照组 40 9.07±1.28 13.94±2.02** 15.90±2.70** 114.09 < 0.01 4.336 t — 0.80 8.50 7.67 — — — P — >0.05 < 0.01 < 0.01 — — — -
2组术前血清NE、Ang-Ⅱ、Cor水平比较差异均无统计学意义(P>0.05);2组术后1 d、3 d时血清NE、Ang-Ⅱ、Cor水平均较术前增高(P < 0.01),但IMN组均低于对照组(P < 0.01)(见表 5)。
分组 n 术前 术后1 d 术后3 d F P MS组内 NE/(ng/L) IMN组 40 221.93±25.19 257.19±29.07** 249.06±27.42** 18.33 < 0.01 743.819 对照组 40 224.52±22.30 289.26±32.24** 274.79±30.48** 59.19 < 0.01 821.913 t — 0.49 4.67 3.97 — — — P — >0.05 < 0.01 < 0.01 — — — Ang-Ⅱ/(ng/L) IMN组 40 45.28±4.41 58.60±5.72** 56.14±4.82** 79.95 < 0.01 25.133 对照组 40 46.47±5.09 67.52±7.38** 63.35±6.27** 124.56 < 0.01 39.895 t — 1.12 6.04 5.77 — — — P — >0.05 < 0.01 < 0.01 — — — Cor/(ng/mL) IMN组 40 204.07±18.16 239.37±24.64** 227.15±21.75** 27.35 < 0.01 469.993 对照组 40 206.10±20.38 257.64±28.39** 241.24±25.47** 44.49 < 0.01 623.353 t — 0.47 3.07 2.66 — — — P — >0.05 < 0.01 < 0.05 — — — 组内配对t检验:与术前比较**P < 0.01 -
2组术前血清ALP、N-MID、β-CTX水平比较差异均无统计学意义(P>0.05);2组术后1周及1个月ALP、N-MID水平均较术前增高,β-CTX水平较术前降低(P < 0.01),且IMN组ALP、N-MID水平高于对照组,β-CTX水平均低于对照组(P < 0.01)(见表 6)。
分组 n 术前 术后1周 术后1个月 F P MS组内 ALP/(U/L) IMN组 40 60.48±7.35 78.09±9.08** 85.36±12.74** 65.73 < 0.01 99.592 对照组 40 59.17±6.46 65.26±7.57** 76.02±10.69** 40.95 < 0.01 71.104 t — 0.85 6.86 3.55 — — — P — >0.05 < 0.01 < 0.01 — — — N-MID/(pg/mL) IMN组 40 28.40±2.07 31.62±2.80** 32.47±3.04** 25.89 < 0.01 7.122 对照组 40 27.62±2.25 29.48±2.52** 30.59±2.73** 14.33 < 0.01 6.289 t — 1.61 3.59 2.91 — — — P — >0.05 < 0.01 < 0.01 — — — β-CTX/(pg/mL) IMN组 40 504.67±57.24 206.38±28.17** 187.29±26.37** 797.72 < 0.01 1 588.448 对照组 40 498.71±51.26 369.56±40.22** 245.42±32.14** 364.69 < 0.01 1 759.405 t — 0.49 21.02 8.84 — — — P — >0.05 < 0.01 < 0.01 — — — 组内配对t检验:与术前比较**P < 0.01 -
经术后6个月随访,IMN组、对照组各有1例病例脱落。IMN组术后6个月Johner-Wruhs功能评分优良率高于对照组(P < 0.05)(见表 7)。
分组 n 差 可 良 优 优良率 χ2 P IMN组 39 0(0.00) 2(5.13) 13(33.33) 24(61.54) 37(94.87) 对照组 39 3(7.69) 7(17.95) 14(35.90) 15(38.46) 29(74.36) 6.30 < 0.05 合计 78 3(3.85) 9(11.54) 27(34.62) 39(50.00) 66(84.62) 注:已排除脱落病例 -
IMN组术后6个月膝关节功能优良率高于对照组(P < 0.05)(见表 8)。
分组 n 差 可 良 优 优良率 χ2 P IMN组 39 0(0.00) 1(2.56) 11(28.21) 27(69.23) 38(97.44) 对照组 39 2(5.13) 6(15.38) 14(35.90) 17(43.59) 31(79.49) 4.52 < 0.05 合计 78 2(2.56) 7(8.97) 25(32.05) 44(56.41) 69(88.46) 注:已排除脱落病例
2.1. 手术情况
2.2. 并发症
2.3. 血清炎症反应指标水平
2.4. 血清应激反应指标水平
2.5. 血清ALP、N-MID、β-CTX水平
2.6. Johner-Wruhs功能评分优良率
2.7. 膝关节功能优良率
-
外科手术为治疗胫骨中下段骨折重要手段,切开复位有限接触钢板内固定、IMN均为重要治疗术式,但关于两者的治疗效果与安全性孰优孰劣临床尚存在一定争议。切开复位有限接触钢板内固定可于直视下实现解剖复位,治疗效果肯定,但笔者发现,切开复位有限接触钢板内固定手术切口较大,术中对软组织剥离较广泛,且对骨膜会造成一定破坏,手术创伤较重,也不利于术后恢复及切口愈合,增加延迟愈合或不愈合、感染、膝关节疼痛、切口皮缘坏死等并发症发生率。陈森荣等[8]研究也报道,应用切开复位有限接触钢板存在创伤重、术后骨折愈合及恢复慢的缺陷。
随现代快速康复理念的发展,临床越来越重视手术的微创性与术后恢复情况。髓内钉技术主要是应用髓内固定原理,为长管状骨骨折提供了治疗新思路。张鑫等[9]研究证实,IMN应用于胫骨中下段骨折病人可显著减少并发症,促进功能恢复。本研究发现,IMN组切口长度、术后下地时间、骨折愈合时间均短于对照组,术中出血量、术后引流量、术后24 h患侧小腿中段周径/术前周径比值、并发症发生率均低于对照组,术后6个月踝关节、膝关节功能恢复优良率均高于对照组。这表明应用IMN治疗具有出血少、术后恢复快、并发症少、功能恢复良好等优势,符合快速康复外科理念。考虑原因为,IMN手术入路微创,可采取闭合穿钉技术,一般情况下不需切开显露骨折端,可避免对骨膜及软组织的广泛剥离,减轻手术创伤,保护骨折断端血供及骨滋养动脉,有助于骨痂形成,且扩髓处理时会产生内植骨效应,利于促进骨折愈合;对软组织剥离少,手术创伤较轻,也利于减少术中出血量与术后引流量,减轻术后患肢肿胀情况,为早期训练创造条件;同时,其力学稳定性良好,并能避免应用钢板固定造成的“应力遮挡”,也利于病人术后早期进行下肢功能锻炼与下地负重训练,促进踝关节、膝关节功能恢复;手术切口小,术中密闭性良好,术后恢复与骨折愈合快,还有助于降低延迟愈合或不愈合、感染、膝关节疼痛、切口皮缘坏死等并发症发生风险[10-11]。
此外,炎症应激反应不仅关系到病人围手术期安全,且与病人术后康复速度、康复效果等有关,在骨折复位固定治疗同时,有效控制不良炎症应激情况也为临床关注重点[12-13]。TNF-α、IL-8、IL-6均为介导应激发生进展过程的重要炎症因子,当机体产生组织损伤或炎症应激状态时,其表达可显著增高[14-16]。NE、Ang-Ⅱ、Cor均为应激激素,其增高幅度与机体应激反应程度呈显著正相关[17]。本研究发现,IMN组术后1 d、3 d血清TNF-α、IL-8、IL-6、NE、Ang-Ⅱ、Cor水平均低于对照组, 表明应用IMN治疗机体炎症应激反应较轻。推测原因可能与IMN手术切口小,对软组织剥离少,创伤轻有关。骨代谢平衡状况可对骨折断端愈合情况产生直接影响,于骨折内固定术后机体会产生代偿性骨吸收抑制与骨形成增加,骨吸收程度和骨折愈合不良风险呈正相关,骨形成强度和骨折愈合不良风险、愈合时间呈明显负相关[18]。ALP、N-MID均与成骨细胞密切相关,表达与成骨过程活跃程度呈正相关,β-CTX为破骨细胞分泌标志物,表达与破骨细胞活性度呈线性相关[19-20]。本研究发现,IMN组术后1周及1个月ALP、N-MID水平高于对照组,β-CTX水平低于对照组, 表明应用IMN治疗术后ALP、N-MID、β-CTX等骨代谢指标恢复快,也从实验室指标层面证实应用IMN治疗具有术后骨折愈合快的优势。但需注意的是,IMN手术操作存在一定难度,要求手术医生具备娴熟的手术操作技术与丰富手术经验,保证手术顺利进行;且在术中应重视断端的短缩移位与旋转,在复位时进行纠正,以保证术后肢体功能恢复效果。
综上,IMN应用于胫骨中下段骨折病人具有出血少、术后恢复快、并发症少、功能恢复良好等优点,且机体炎症应激反应程度轻,骨代谢指标恢复快。
 DownLoad:
DownLoad: