

-
消化道黏膜下肿瘤(submucosal tumor, SMT)是指消化道上皮以下组织起源的实体性肿瘤,常见的SMT包括间平滑肌瘤、质瘤、静脉瘤、神经内分泌肿瘤、脂肪瘤、异位胰腺等[1]。随着内镜技术的进步及不断完善,镜下治疗和超声内镜诊断技术的普及和推广应用,SMT的早诊率逐年提高。以往对于SMT的治疗以外科手术为主,但外科手术存在创伤性大、并发症多、术后恢复时间长等缺点。内镜下黏膜剥离术(endoscopic submucosal dissection, ESD)及全层切除术(Endoscopic full-thickness resection, EFR)是近年快速发展的内镜下微创治疗技术[2]。HOSOKAWA等[3]最早应用ESD技术进行早期胃癌的内镜下治疗,近年随着ESD技术在中国的开展普及,临床医师的经验提高,已逐渐应用于黏膜下层较大肿瘤的切除。其过程是利用电刀对病变组织进行完整剥离,较大的病变甚至可以进行全层切除,术后的病灶组织可以进行完整的病理诊断及分期,对于临床医师准确判断预后及制定进一步治疗措施有很大帮助[4]。此外,对于来源于固有肌层的黏膜下肿瘤还可以进行较深的全层切除,再用金属钛夹完整封闭创口,从而避免外科开腹手术[5]。食管、胃及十二指肠的常见SMT病灶是平滑肌瘤、间质瘤等,大多数是良性病变,但存在恶性变的潜质。目前临床已基本达成了SMT首选ESD治疗的共识[6]。我院自2013年开展ESD技术,2014年成功应用ESD及EFR技术治疗上消化道SMT,本研究回顾性分析我院接受ESD及EFR技术治疗的197例上消化道SMT病例情况。现作报道。
-
回顾性收集2016年12月至2019年12月在我院住院治疗并行ESD或EFR治疗的上消化道SMT病人197例。其中男85例,女112例;年龄17~76岁;病灶位于食管70例,贲门1例,胃底35例,胃体28例,胃窦56例,十二指肠7例。所有病人均经内镜检查怀疑黏膜下肿瘤,经超声内镜及CT再次检查后初步判断病变性质、确认病变层次和范围。所有病人均在术前告知其ESD或EFR手术可能的获益和相关风险,并要求病人签署手术知情同意书。
-
采用Olympus GIF-Q260J电子胃镜、KD650-Q Dual刀、KD-610LIT刀、KD-620LR Hook刀、FD-410LR热活检钳、NM24L21注射针、ERBE VIO 200s+APC2高频电切装置和氩离子凝固器、SP-210U-25电圈套器、ROCC-D-26-195金属夹等器材器械辅助手术。此外,ESD治疗过程中所使用的内镜头端均需附加透明帽。
-
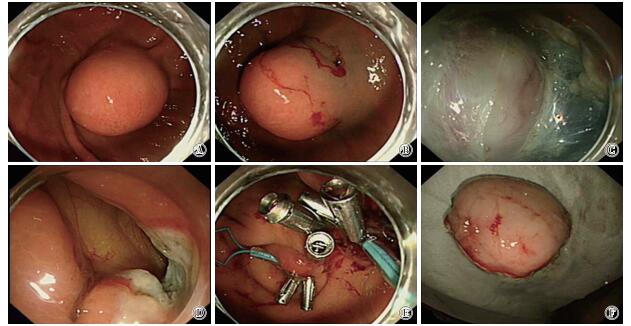
术前完善血常规、凝血、心电图及胸部、上腹部CT检查,所有病人均行全麻气管插管辅助ESD手术。(1)手术标记:应用针形切开刀或氩离子凝固术(APC术)在病灶边缘0.5~1 cm处进行电凝标记;(2)注射:混合0.4%靛胭脂2 mL和0.9%氯化钠溶液250 mL,在标记点外侧进行环周黏膜下层注射使病变抬举;(3)切开:应用Dual刀、Hook刀或IT刀沿上述标记点切开黏膜及黏膜下层;(4)剥离及切除:采用联合应用各种切开刀对黏膜下层和肿瘤外缘之间进行剥离,剥离应沿病变基层切线方向,剥离过程中一般需要反复多次地进行黏膜下注射才能使病变抬举良好,对于瘤体侵及固有肌层及浆膜层的病变,需进行“主动穿孔”完整切除肿瘤;(5)剥离后创面处理:切除病灶后,如创面有可见的小血管,需利用热活检钳或APC进行止血处理,必要时联合应用金属钛夹封闭创面。全层切除的病灶利用金属钛夹及尼龙绳行荷包缝合术封闭创面[8](见图 1)。

图 1 胃底间质瘤的EFR
-
切除病灶展评并用细针固定,浸泡于4%多聚甲醛溶液固定,及时送病理检查及免疫组织化学检查确定病变的病理性质,病理检查需密切观察病灶的基底部和边缘有无病变侵及。病人术后第1~2天禁食水,常规使用质子泵抑制剂抑酸、止血药物及营养支持治疗,EFR病人需额外给予抗生素治疗,并严密观察有无腹痛、腹胀等腹部体征[9]。术后第3~4天如无腹痛、腹胀、出血等特殊不适症状,可开始进流质,逐步过渡至正常饮食。术后1、3、6个月常规复查内镜和/或超声内镜,复查时注意观察创面的愈合情况,同时注意观察有无病灶局部的残留、复发。
-
采用t检验。
-
197例上消化道SMT病人中,154例经ESD手术一次完整剥离成功,病灶直径0.8~3.0 cm,ESD手术时间(病灶标记至完整剥离成功)15~31 min,术后住院时间3~7 d。43例病灶起源于固有肌层及固有肌层与浆膜紧密粘连,其中26例位于胃底,15例位于胃体,1例位于胃窦,1例位于十二指肠,均接受EFR。其中1例因瘤体大、粘连,术中剥离困难,中转外科行腹腔镜治疗,其他42例病灶直径1.2~4.0 cm,手术时间41~134 min,术后住院时间5~10 d。ESD组病灶直径、手术时间、住院时间均明显小于EFR组(见表 1)。
分组 n 病灶直径/cm 手术时间/min 住院时间/d ESD组 154 1.5±0.5 24.0±3.6 4.9±1.5 EFR组 43 1.9±0.8 52.0±9.7 6.7±1.8 t — 4.01 29.43 6.65 P — < 0.01 < 0.01 < 0.01 表 1 行ESD和EFR病人病灶直径、手术时间及住院时间比较(x±s)
并发症方面,3例术中有少量出血,均经内镜下电凝APC和金属钛夹成功止血;未出现ESD及EFR术中或术后大出血。154例ESD术中均无穿孔;43例EFR术中均主动穿孔,包括5例平滑肌瘤,38例固有肌深层来源的间质瘤。内镜下EFR切除的病灶均经胃镜下金属夹和尼龙绳行荷包缝合成功封闭创面;术后所有病人禁饮食,并给予胃肠减压、质子泵抑制剂抑酸、抗生素、肠外营养支持等保守治疗成功。
术后病理及免疫组织化学明确诊断平滑肌瘤75例、间质瘤39例、异位胰腺43例、脂肪瘤26例、囊肿4例、神经内分泌肿瘤3例、神经鞘瘤3例、腺肌瘤2例、血管瘤1例及淋巴管瘤各1例。随访3~18个月,中位随访时间7个月,均无病变复发。
-
随着超声内镜技术的开展和普及,消化道黏膜下肿瘤的早诊率逐年提高[10]。大多黏膜下肿瘤为良性肿瘤,上消化道黏膜下肿瘤中以平滑肌瘤最为常见,这与我们的研究结果一致[11]。关于较为常见的间质瘤,普遍认为起源于固有肌层的间质瘤具有潜在恶变的特质。既往观点认为仅起源于黏膜下层的SMT可行内镜下切除,起源于固有肌层或与浆膜层粘连紧密的病灶难以经内镜下切除,且容易出现出血、穿孔等并发症,因此间质瘤等病灶多采取定期随访或创伤更大的外科手术[12]。随着镜下治疗的飞速发展,ESD及EFR技术的成熟使深层的消化道SMT内镜下完整安全地切除成为可能,且这两种微创技术可为临床医师提供完整的病理诊断,从而制定更加优化的进一步治疗或随访策略[13-14]。
本研究回顾性总结了上消化道SMT病例197例,结果显示,ESD及EFR可以一次性完整剥离多数来源于黏膜下层的 < 4 cm的SMT,包括平滑肌瘤、间质瘤、脂肪瘤等。与外科手术相比,病人术后恢复快,住院时间短,医疗费用低,充分展现了内镜下微创治疗的优越性[15]。
安全性方面,出血和穿孔是ESD及EFR的主要手术并发症。对于出血而言,应首选内镜下止血,对于内镜下止血困难的病例需果断中止手术,转外科手术治疗。在处理肿瘤创面时应较剥离时更加小心,尤其是对于起源于固有肌层的病变,剥离完毕后残余的固有肌层或浆膜层非常薄,电凝处理血管时稍不注意即有穿孔的可能[16]。穿孔方面,本研究中共43例发生穿孔,均为主动穿孔。原因是这些病灶来源于固有肌层或向外生长,或与浆膜层紧密粘连,要完整剥离病灶很难避免穿孔[17],临床往往采用主动穿孔,即EFR。本组43例固有肌层间质瘤向外生长,因此采用内镜下全层切除术,术后使用金属夹尼龙圈荷包缝合法成功实施了创面封闭。术后给予禁饮食、胃肠减压、抑制胃酸分泌、抗感染、营养支持等对症处理。
ESD或EFR治疗SMT的适应证应严格把握。目前观点认为较大的间质瘤(>3 cm)不宜采用内镜下微创治疗技术。消化道间质瘤主要来源于肌层,是一种侵袭性肿瘤,生物学行为较难预测,有观点[18]认为3 cm以下的间质瘤可定期随访,而肿瘤直径>5 cm时伴随远处转移和消化道出血的概率增高,主张外科手术切除。对于来源于固有肌层的间质瘤,则应根据超声内镜下的风险分级综合判断,不良因素包括表面溃疡、边界不规整、异质性和强回声等[19]。此外,应用ESD或EFR治疗神经内分泌肿瘤需要谨慎术前评估,对于肿瘤分级高、存在淋巴管浸润的病人需评估是否同时伴有其他器官转移,本研究中发现的3例神经内分泌肿瘤术后病理分级为G1级,未转外科继续治疗[20]。
综上,ESD及EFR技术的快速发展使消化道SMT的内镜下微创切除成为可能,并能在不破坏正常生理解剖结构的前提下提供全面的病理诊断,具有创伤性小、术后恢复快、术中及术后并发症发生率低、花费少等优点。但该项技术对内镜操作者技术要求标准较高,应在有条件的医院由经验丰富的内镜医师循序渐进开展才能取得良好效果,同时也需要严格把握该手术的适应症及注意术后定期随访。
内镜黏膜下剥离术及全层剥离术治疗上消化道黏膜下肿瘤197例分析
Value of endoscopic submucosal dissection and endoscopic full-thickness resection in the treatment of upper gastrointestinal submucosal tumors:197 cases analysis
-
摘要:
目的探讨内镜黏膜下剥离术(endoscopic submucosal dissection,ESD)及全层剥离术(endoscopic full-thickness resection,EFR)治疗上消化道黏膜下肿瘤的有效性及安全性。 方法回顾性分析消化科住院治疗的上消化道黏膜下肿瘤病人197例,均接受ESD或EFR手术,统计治疗切除率、手术时间、术中穿孔率、术后出血率及术后病理情况。 结果197例中154例起源于黏膜下层,行ESD治疗,均完整剥离病灶,ESD平均手术时间(病灶标记至完整剥离成功)为(24.0±3.6)min;所有ESD病人术后均无出血发生,术中均无穿孔,均经金属钛夹成功封闭创面。43例起源于固有肌层及与浆膜层紧密粘连,遂行EFR。42例一次完整剥离成功,均经胃镜下金属钛夹及尼龙绳荷包缝合成功封闭创面;1例因瘤体较大,病变粘连、剥离困难,改用外科手术。EFR平均手术时间为(52.0±9.7)min,术后均无出血发生,术中均主动穿孔。ESD或EFR术后病理及免疫组织化学诊断为平滑肌瘤75例、异位胰腺43例,间质瘤39例、脂肪瘤26例,囊肿4例、神经内分泌肿瘤3例,神经鞘瘤3例、腺肌瘤2例,血管瘤1例、淋巴管1例。术后随访3~18个月,中位随访时间7个月,均未复发。 结论ESD及EFR技术可以安全完整切除上消化道黏膜下肿瘤,并提供完整可靠的病理诊断,具有创伤小、恢复快的优点,值得临床进一步推广。 Abstract:ObjectiveTo assess the efficacy and safety of endoscopic submucosal dissection(ESD) and endoscopic full-thickness resection(EFR) in the treatment of the upper gastrointestinal submucosal tumors(SMT). MethodsThe clinical data of 197 patients with upper gastrointestinal SMT were retrospectively analyzed.All patients were treated with ESD or EFR.The tumor resection rate, operation time, intraoperative perforation rate, postoperative bleeding rate and histopathological results in the patients were evaluated. ResultsAmong the 197 patients, 154 cases originated from submucosa, were treated with ESD, and the lesions were completely stripped.The average operative time(from lesion labeling to complete dissection) of ESD was (24.0±3.6)min, no postoperative bleeding occurred, the perforation occurred during the operation, and the wound was successfully closed by titanium clips.Forty-three cases originated from submucosa, the tumors tightly adhered to the serous membrane layer, and were treated with EFR.Complete dissections in 42 cases were successfully performed, and the wound was successfully closed by titanium clips and nylon pocketbook suture under gastroscope.One case was changed to surgical operation due to the large tumor body and difficulty in adhesion and dissection.The mean operation time of EFR was (52.0±9.7)min, no hemorrhage occurred after operation, and the aortic perforation in the patients were found during EFR.The results of pathological and immunohistostaining examination identified the leiomyoma in 75 cases, ectopic pancreas in 43 cases, stromal tumor in 39 cases, lipoma in 26 cases, cyst in 4 cases, neuroendocrine tumor in 3 cases, schwannoma in 3 cases, adenomyoma in 2 cases, hemangioma in 1 case and lymphangioma in 1 case.All patients were followed up for 3 to 18 months, the median follow-up time was 7 months, and there was no recurrence case. ConclusionsESD and EFR technology can safely and completely remove the upper gastrointestinal SMT, and provide a complete and reliable pathological diagnosis.With the advantages of small trauma and quick recovery, it is worthy of further clinical promotion. -
表 1 行ESD和EFR病人病灶直径、手术时间及住院时间比较(x±s)
分组 n 病灶直径/cm 手术时间/min 住院时间/d ESD组 154 1.5±0.5 24.0±3.6 4.9±1.5 EFR组 43 1.9±0.8 52.0±9.7 6.7±1.8 t — 4.01 29.43 6.65 P — < 0.01 < 0.01 < 0.01  下载: 导出CSV
下载: 导出CSV
-
[1] 武绍梅, 郑苏云.内镜下黏膜剥离术在胃肠道疾病中的应用[J].临床医药文献杂志, 2016, 3(29):5909. [2] 蔡明琰, 诸炎, 周平红.内镜微创治疗——由表及里, 由内而外[J].中华胃肠外科杂志, 2019, 22(7):601. [3] HOSOKAWA K, YOSHIDA S.Recent advantages in endoscopic mucosal resection for early gastric cancer[J].GanTo Kagaku Ryoho, 1998, 25(4):476. [4] KIM SG, PARK CM, LEE NR, et al.Long-term clinical outcomes of endoscopic submucosal dissection in patients with early gastric cancer:A prospective multicenter cohort study[J].Gut Liver, 2018, 12(4):402. doi: 10.5009/gnl17414 [5] 姚健, 王军, 马俊等.内镜下全层切除术治疗胃固有肌层间质瘤的临床疗效分析[J].实用临床医药杂志, 2017, 21(9):131. [6] CHUNG MW, JEONG O, PARK YK, et al.Comparison on the long term outcome between endoscopic submucosal dissection and surgical treatment for undifferentiated early gastric cancer[J].Korean J Gastroenterol, 2014, 63(2):90. doi: 10.4166/kjg.2014.63.2.90 [7] CHUNG IK, KIM HJ, LEE SH, et al.Therapeutic outcome in 1000 cases of endoscopic submucosal dissection (ESD) for early gastric neoplasms; Korean ESD Study Group (KESG) multi-center study[J].Gastrointest Endosc, 2008, 67(5):AB94. [8] 钟芸诗, 时强, 姚礼庆, 等.内镜全层切除术后胃壁缺损的金属夹联合尼龙绳简短缝合术[J].中华胃肠外科杂志, 2012, 15(3):280. [9] NISHIZAWA T, SUZUKI H, AKIMOTO T, et al.Effects of preoperative proton pump inhibitor administration on bleeding after gastric endoscopic submucosal dissection:a systematic review and meta-analysis[J].United European Gastroenterol J, 2016, 4(1):5. doi: 10.1177/2050640615588023 [10] 吴巍, 范嵘, 谭继宏, 等.内镜超声对消化道黏膜下肿瘤内镜术前评估的价值和局限性[J].中华消化内镜杂志, 2019, 36(7):491. [11] 彭金榜, 叶丽萍, 毛鑫礼, 等.上消化道黏膜下肿瘤1237例次的病理学特征和分布特点[J].中华消化杂志, 2019, 39(2):94. [12] 周平红, 徐美东, 陈巍峰, 等.内镜黏膜下剥离术治疗直肠病变[J].中华消化内镜杂志, 2007, 24(1):40. [13] 张月明, 王贵齐.内镜黏膜切除及黏膜下剥离术的并发症处理及预防[J].中华消化内镜杂志, 2008, 25(11):567. [14] GAMBITTA P, LANNUZZI F, BALLERINI A, et al.Endoscopic submucosal dissection versus endoscopic mucosal resection for type 0-Ⅱ superficial gastric lesions larger than 20mm[J].Ann of Gastroenterol, 2018, 31(S1):338. [15] 时强, 钟芸诗, 姚礼庆.内镜全层切除术的研究进展[J].中华消化内镜杂志, 2011, 28(10):595. [16] 金晶.内镜黏膜下剥离术治疗胃肠道间质瘤的分析[J].医药前沿, 2016, 6(7):85. [17] 张周娟, 骆泉.内镜黏膜下剥离术治疗胃肠道间质瘤术中穿孔的危险因素分析[J].北京医学, 2018, 40(6):562. [18] SAKURA Y, SAKURAI S.Molecular characteristics of GISTs[J].Stomach Intestine, 2004, 39(4):405. [19] 任春蓉, 孙晓滨, 史维, 等.内镜黏膜下剥离术治疗消化道黏膜下肿瘤43例分析[J].实用医院临床杂志, 2015, 12(5):172. [20] 王小云, 徐美东, 周平红, 等.内镜黏膜下剥离术治疗上消化道神经内分泌肿瘤的临床价值[J].中华消化内镜杂志, 2012, 29(12):679. -

 点击查看大图
点击查看大图
图(1)表(1)
计量
- 文章访问数: 5039
- HTML全文浏览量: 2387
- PDF下载量: 13
- 被引次数: 0
