


-
选取2010年1月至2018年1月在蚌埠医学院第一附属医院接受胃癌手术的45岁以上病人。外科医师进行了所有胃癌手术,并且由一组胃肠病理学家进行了组织学检查。收集临床病理数据,包括人口统计学信息、手术数据、肿瘤分期和生存状态。根据美国癌症联合委员会(AJCC)(第8版)TNM标准对病理阶段进行了分类[5-7]。T分期(T1,肿瘤侵袭固有层,肌层黏膜或黏膜下层;T2,肿瘤侵犯固有肌层;T3,肿瘤穿透浆膜下结缔组织而没有侵犯脏腹膜或邻近结构;T4a,浆膜(脏腹膜)的肿瘤侵袭;T4B, 肿瘤侵犯邻近结构、器官), N分期(N0, 无区域淋巴结转移;N1,1~2个淋巴结转移;N2,转移3~6个区域淋巴结;N3a,7~15个区域淋巴结转移;N3b,≥16个区域淋巴结转移)。本研究共纳入236例病人。排除标准:(1)缺乏组织学诊断;(2) 原发肿瘤不需手术切除;(3) 既往或并发恶性肿瘤病史;(4)原位癌或远处转移;(5) 无阳性淋巴结计数和/或检查淋巴结总数记录;(6)术前放射治疗。
-
根据我们的标准方案进行定期随访,对于早期和晚期胃癌,术后3年每6个月和3个月随访一次,3年后每12个月随访一次。包括肿瘤标志物水平、腹部计算机断层扫描和内镜检查。观察期是指从手术日期到死亡或丧失随访之间的时间间隔,以先到者为准。计算总生存期(OS),从胃切除术日期到因任何原因导致的死亡日期或最后一次随访日期。平均随访时间为36个月。该研究方案由蚌埠医学院的机构审查委员会批准。在分析之前,对病人记录进行匿名和取消标识。
-
采用线性回归分析、Kaplan-Meier法、对数秩检验、Cox比例风险模型和logistic回归分析。
-
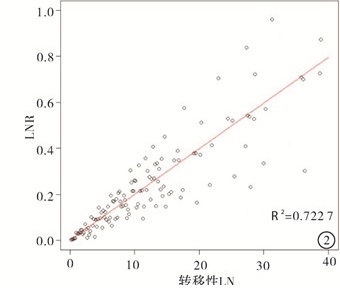
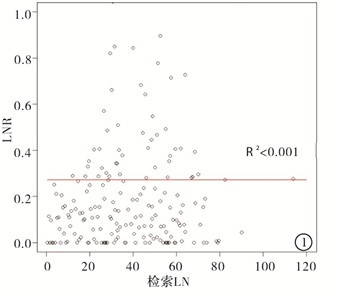
散点图显示LNR与解剖的LN数量之间无相关性(R2 < 0.001)。但是,LNR和转移性LN的数量之间存在线性关系(R2=0.722 7)。LNR随着转移性LN数量的增加而增加(见图 1、2)。

图 1 NR与检索到的LN数量之间的相关性

图 2 LNR与转移性LN数量之间的相关性.
-
在入组病人中,男159例(67.38%),女77例(32.62%)。开放方式(77.12%)比腹腔镜方式(22.88%)更频繁,远端胃切除术是最常见的手术范围(193例,占81.78%)。按LN解剖分类时,有115例(48.72%)的病人接受了D0或D1解剖,而121例(51.28%)的病人进行了D2或以上解剖。根据TNM分期,有118例病人(50.00%)患有Ⅰ期肿瘤,62例(26.27%)具有Ⅱ期肿瘤,56例(23.73%)具有Ⅲ期肿瘤。平均肿瘤直径为4.7 cm,平均回收的LN数为37.3±12.9(见表 1)。
变量 类别 数量和平均值 年龄/岁 67.9±5.2 性别 男 159 女 77 体质量指数/(kg/m2) 23.6±2.8 手术方式 腔镜 54 开放 182 切除范围 全胃 42 远端胃 193 近端胃 1 LN清扫范围 <D2 115 >D2 121 估计失血量/mL 135.7±109.6 手术时间/min 172.3±59.2 肿瘤大小/cm 5.8±4.1 淋巴结个数 37.3±12.9 T分期* T1 44 T2 40 T3 47 T4 105 N分期* N0 102 N1 49 N2 39 N3 46 TNM分期* Ⅰ 118 Ⅱ 62 Ⅲ 56 治疗方式 根治性切除 227 姑息性切除 9 *根据美国癌症联合委员会(第8版)TNM标准分类的病理分期 表 1 临床病理特征
-
结果显示,OS随着N阶段和LNR阶段的增加而显著下降。但是,对于LNR分期,各阶段之间生存率的增量变化大于常规的N分期(P < 0.01)(见图 3)。

图 3 按N分期和LNR分期分层的老年胃癌病人OS的Kaplan-Meier曲线
-
对于基于LNR的生存分析,本研究使用0.1的间隔将LNR分为11组,分析每组的3年和5年OS率,并根据风险比(HR)增加的拐点将11组分为4个基于LNR的阶段。LNR阶段0(LNR0)对应于0的LNR,并用作参考水平。LNR阶段1(LNR1)包括介于0和0.1之间的LNR值。第2阶段(LNR2)包括从0.1到0.6的LNR值,其中HR为4.157。第3阶段(LNR3)包括高于0.6的LNR值,此时HR突然增加到17.452。在纳入的病人中,将89例病人分类为LNR0,将47例病人分类为LNR1,将90例病人分类为LNR2,将10例病人分类为LNR3(见表 2)。分类为每个LNR分期和相应N分期的病人数量见表 3。
LNR分期 LNR分组 数量 3年OS/% 5年OS/% HR 95%CI 0 LNR=0 89 87.2 76.5 Ref 1 0 < LNR≤0.1 47 69.4 57.1 1.824 1.275~2.642 2 0.1 < LNR≤0.2 39 47.3 25.7 4.157 3.183~7.012 0.2 < LNR≤0.3 17 23.4 11.6 5.853 3.072~9.046 0.3 < LNR≤0.4 21 39.8 7.53 7.904 4.481~17.526 0.4 < LNR≤0.5 11 31.8 12.7 4.978 2.043~10.164 0.5 < LNR≤0.6 2 42.4 18.6 5.703 3.298~17.034 3 0.6 < LNR≤0.7 3 0 0 17.452 7.344~42.831 0.7 < LNR≤0.8 4 0 0 22.367 5.268~87.259 0.8 < LNR≤0.9 2 0 0 18.517 3.798~113.562 0.9 < LNR≤1.0 1 0 0 35.842 11.948~128.474 表 2 每个LNR组的3年和5年OS
LNR分期 LNR分组 总数量 N分期 分数量 0 LNR=0 89 N0 89 1 0<LNR≤0.1 47 N1 39 N2 7 N3 1 2 0.1<LNR≤0.6 90 N1 8 N2 19 N3 53 3 0.6<LNR≤1.0 10 N2 2 N3 8 表 3 LNR分期与常规N分期的组成
-
在传统的T分期中,T2和T4阶段是OS的重要预测指标(T2:HR 1.529,95%CI 1.063~2.837,P < 0.05;T4:HR 2.746,95%CI 1.832~3.734,P < 0.01)。在多因素分析中,N期和LNR期是生存预后的重要预后因素。但是,LNR分期的各阶段HR的变化要大于N分期(N分期的HR:1.583、2.789和4.581;LNR分期的HR:分别为1.469、3.837和8.572)(见表 4)。
变量 HR 95%CI P 性别 1.185 0.792~1.198 >0.05 T分期 T1 Ref. < 0.01 T2 1.529 1.063~2.837 >0.05 T3 1.316 0.936~1.769 >0.05 T4 2.746 1.832~3.734 < 0.01 N分期 N0 Ref. < 0.01 N1 1.583 1.038~2.874 < 0.01 N2 2.789 1.376~5.013 < 0.01 N3 4.581 2.183~6.384 < 0.01 LNR分期 LNR0 Ref. < 0.01 LNR1 1.469 0.932~2.517 < 0.01 LNR2 3.837 2.376~4.095 < 0.01 LNR3 8.572 5.619~17.237 < 0.01 表 4 OS多变量分析结果
-
准确的分期对于预测胃癌病人的预后很重要[8-9]。我国胃癌发病年龄主要集中在45岁以上,在对病人TNM分期的分析中发现,除了少数早期胃癌,青年(< 45岁)和45岁以上在TNM分期上存在显著差异。青年TNM主要集中于Ⅳ期,而45岁以上病人主要集中于Ⅲ期和Ⅳ期。青年中Ⅱ期的构成比要低于45岁以上,而Ⅳ期的构成比要高于45岁以上病人[10-11]。美国癌症联合委员会(AJCC) 和国际癌症控制联盟(UICC)合作建立的最新版本TNM分期中最高级阶段(N3b)要求至少切除16个淋巴结以确定N分期,TNM系统正确分期似乎取决于淋巴结清扫的范围[12-15]。由于LNR不受回收的LN数量的影响,因此当广泛的LN解剖对身体有害时,其是更有利于胃癌分期的。D2 LN解剖是晚期胃癌的标准治疗方法,但是广泛的LN解剖比有限的LN解剖需要更长的手术时间,这会造成大量失血的风险。因此,广泛清扫淋巴结会对患有心血管或呼吸系统疾病和45岁以上病人带来更高的风险,也更容易术后出血及麻醉并发症。与需要至少16个LN的传统TNM分期相比,在需要有限LN解剖的情况下,LNR分期具有一定的临床应用价值。美国麻醉医师协会目前对存在基础疾病,影响正常生活的病人开始使用LNR分期进行病情评估。
在本研究中,我们使用新定义的LNR分期对236例45岁以上胃癌病人进行了分类,并分析了他们的生存率。在不同的N分期和LNR分期阶段之间,发现生存率存在显著差异。为了消除可能影响生存率的潜在混杂因素,我们进行了多变量分析,结果显示N分期和LNR分期是病人预后的重要预测指标。迄今为止,大多数涉及LNR的研究都使用一个临界值将病人分为两个LNR组。然而,不同的研究提出了不同的临界值,并且没有提出正式标准来代替N阶段。本研究的优势之一是LNR分组和使用三个特定的临界值进行后续分期。这些值遵循与常规N分期相似的分类,因此易于在临床实践中应用。我们最初选择的临界值为0,并将所有病人分为LNR=0和LNR>0组。随后我们根据HR的变化确定了临界值0.1和0.6。此过程包括4个LNR阶段:LNR0,LNR1,LNR2和LNR3,与N分级系统中的数目相同。LNR分期概念可以在临床实践中以类似于N分期的方式应用,可能是评估45岁以上胃癌病人预后的有效新方法。
本研究的局限性包括这是一项回顾性单中心研究,因此存在选择偏倚的可能性。另外我们根据Cox比例风险模型中的HR划分了阶段,没有采用更精确的统计方法。但是与当前的N分期系统类似,我们纳入了相对大量的病人,并生成了足够的数据来获取区分四组的临界值。这是一项评估类似于常规N分期的LNR分期在45岁以上胃癌病人中有用性的研究。基于这项研究的结果,我们提出了一个新的类似于N分期的LNR分期系统。本研究发现LNR分期在预测可能需要有限LN解剖的45岁以上胃癌病人的预后方面具有一定的临床实用价值。未来包括需要有限淋巴结清扫的更大病人群在内的进一步研究可能有助于确定LNR分期在临床实践中的实用性。
基于淋巴结比率的45岁以上病人胃癌分期的新方法
A new method for staging gastric cancer in patients over 45 years old based on the lymph node ratio
-
摘要:
目的评估淋巴结比率(LNR)作为45岁以上胃癌病人分期评估的实用性。 方法接受根治性胃切除术的45岁以上病人236例,收集包括回收的淋巴结(LN)和转移性淋巴结(LNs)的临床病理数据,并计算LNR值(LNR=LNs/LN)。根据危险比(HR)增加的截止点,将间隔为0.1的LNR组分为4个阶段。进行生存分析以评估LNR的预后价值。 结果4个LNR级包括LNR0(n=89),LNR1(n=47),LNR2(n=90)和LNR3(n=10)。在多变量分析中,N分期和LNR分期均显示出显著的预后价值,可预测生存结果。LNR分期在连续阶段之间的HR的增量变化大于N分期(HR:N分期为1.583、2.789和4.581;LNR分期为1.469、3.837和8.572)。 结论LNR分期作为一种新颖且简单的评估方法,在预测45岁以上胃癌病人的预后和复发方面具有一定的临床应用价值。 Abstract:ObjectiveTo evaluate the utility of lymph node ratio(LNR) in the staging assessment of patients over 45 years old with gastric cancer. MethodsThe patients aged 45 years or older treated with radical gastrectomy were investigated, the clinicopathological data of recovered lymph nodes(LN) and metastatic lymph nodes(LNs) were collected, and the LNR values were obtained(LNR=LNs/LN).The LNR group with 0.1 intervals was divided into four phases based on the cutoff point of increased hazard ratio(HR).The survival analysis was performed to assess the prognostic value of LNR. ResultsThe four LNR levels included the LNR0(n=89), LNR1(n=47), LNR2(n=90) and LNR3(n=10).In the multivariate analysis, both N staging and LNR staging showed the significant prognostic value, and which could predict the survival outcome.The incremental changes in the HR among successive stages of LNR staging were greater than those of N staging(HR: the N staging was 1.583, 2.789 and 4.581, and the LNR staging was 1.469, 3.837 and 8.572). ConclusionsThe LNR staging, a novel and simple marker, has certain clinical application value in predicting the prognosis and recurrence of gastric cancer in patients over 45 years old. -
Key words:
- gastric neoplasms /
- lymph node ratio /
- prognosis
-
表 1 临床病理特征
变量 类别 数量和平均值 年龄/岁 67.9±5.2 性别 男 159 女 77 体质量指数/(kg/m2) 23.6±2.8 手术方式 腔镜 54 开放 182 切除范围 全胃 42 远端胃 193 近端胃 1 LN清扫范围 <D2 115 >D2 121 估计失血量/mL 135.7±109.6 手术时间/min 172.3±59.2 肿瘤大小/cm 5.8±4.1 淋巴结个数 37.3±12.9 T分期* T1 44 T2 40 T3 47 T4 105 N分期* N0 102 N1 49 N2 39 N3 46 TNM分期* Ⅰ 118 Ⅱ 62 Ⅲ 56 治疗方式 根治性切除 227 姑息性切除 9 *根据美国癌症联合委员会(第8版)TNM标准分类的病理分期  下载: 导出CSV
下载: 导出CSV
表 2 每个LNR组的3年和5年OS
LNR分期 LNR分组 数量 3年OS/% 5年OS/% HR 95%CI 0 LNR=0 89 87.2 76.5 Ref 1 0 < LNR≤0.1 47 69.4 57.1 1.824 1.275~2.642 2 0.1 < LNR≤0.2 39 47.3 25.7 4.157 3.183~7.012 0.2 < LNR≤0.3 17 23.4 11.6 5.853 3.072~9.046 0.3 < LNR≤0.4 21 39.8 7.53 7.904 4.481~17.526 0.4 < LNR≤0.5 11 31.8 12.7 4.978 2.043~10.164 0.5 < LNR≤0.6 2 42.4 18.6 5.703 3.298~17.034 3 0.6 < LNR≤0.7 3 0 0 17.452 7.344~42.831 0.7 < LNR≤0.8 4 0 0 22.367 5.268~87.259 0.8 < LNR≤0.9 2 0 0 18.517 3.798~113.562 0.9 < LNR≤1.0 1 0 0 35.842 11.948~128.474
下载: 导出CSV
表 3 LNR分期与常规N分期的组成
LNR分期 LNR分组 总数量 N分期 分数量 0 LNR=0 89 N0 89 1 0<LNR≤0.1 47 N1 39 N2 7 N3 1 2 0.1<LNR≤0.6 90 N1 8 N2 19 N3 53 3 0.6<LNR≤1.0 10 N2 2 N3 8
下载: 导出CSV
表 4 OS多变量分析结果
变量 HR 95%CI P 性别 1.185 0.792~1.198 >0.05 T分期 T1 Ref. < 0.01 T2 1.529 1.063~2.837 >0.05 T3 1.316 0.936~1.769 >0.05 T4 2.746 1.832~3.734 < 0.01 N分期 N0 Ref. < 0.01 N1 1.583 1.038~2.874 < 0.01 N2 2.789 1.376~5.013 < 0.01 N3 4.581 2.183~6.384 < 0.01 LNR分期 LNR0 Ref. < 0.01 LNR1 1.469 0.932~2.517 < 0.01 LNR2 3.837 2.376~4.095 < 0.01 LNR3 8.572 5.619~17.237 < 0.01
下载: 导出CSV
-
[1] 丁平安, 杨沛刚, 田园, 等. pT1N3M0期胃癌患者的临床病理特征及预后分析[J]. 中华普通外科杂志, 2020, 35(8): 598. doi: 10.3760/cma.j.cn113855-20200226-00128 [2] GAO M, YO G. Value of preoperative neutrophil-lymphocyte ratio and human epididymis protein 4 in predicting lymph node metastasis in endometrial cancer patients[J]. J Obstet Gynaecol Res, 2021, 47(2): 515. doi: 10.1111/jog.14542 [3] 赵哲明, 裴俊鹏, 姜洪磊, 等. 淋巴结比率用于Ⅲ期直肠癌患者的预后评价[J]. 中国医科大学学报, 2020, 49(3): 258. [4] 张怡, 钱萍. 转移性淋巴结比率在淋巴转移胆囊癌患者中的预后意义及预后模型建立[J]. 浙江医学, 2018, 40(20): 2216. doi: 10.12056/j.issn.1006-2785.2018.40.20.2018-2287 [5] 高源, 彭贵勇. 早期胃癌淋巴结转移规律的临床病理因素研究[J]. 中华消化内镜杂志, 2020(4): 257. doi: 10.3760/cma.j.cn321463-20191021-00702 [6] COMAN RT, CRISAN N, KADULA PA, et al. Neutrophil-to-lymphocyte ratio above 2-advocate for lymph node dissection in prostate cancer[J]. J Buon, 2018, 23(1): 275. [7] 程元光, 文刚, 汪毅, 等. 远端胃癌第12组淋巴结廓清术不同手术入路的临床疗效和安全性分析[J]. 蚌埠医学院学报, 2019, 44(6): 721. [8] KUTLU OC, WATCHELL M, DISSANAIKE S. Metastatic lymph node ratio successfully predicts prognosis in western gastric cancer patients[J]. Surg Oncol, 2015, 24(2): 84. doi: 10.1016/j.suronc.2015.03.001 [9] MOUG SJ, OLIPHANT R, BALSITIS M, et al. The lymph node ratio optimises staging in patients with node positive colon cancer with implications for adjuvant chemotherapy[J]. Int J Colorectal Dis, 2014, 29(5): 599. doi: 10.1007/s00384-014-1848-4 [10] ZHU GS, TIAN SB, WANG H, et al. Preoperative neutrophil lymphocyte ratio and platelet lymphocyte ratio cannot predict lymph node metastasis and prognosis in patients with early gastric cancer: a single institution investigation in China[J]. Curr Med Sci, 2018, 38(1): 78. doi: 10.1007/s11596-018-1849-6 [11] 李庆刚, 钱文彪, 胡晓翠, 等. 阳性淋巴结比率对结直肠癌患者预后的预测价值[J]. 临床肿瘤学杂志, 2013, 18(8): 730. doi: 10.3969/j.issn.1009-0460.2013.08.014 [12] OZCAN A, COLLADO DIAZ V, HALIN C, et al. Neutrophil recruitment to local and systemic lymph nodes is differentially guided in inflammation[J]. Allergy, 2020, 75(6): 287. [13] BOGOSLOWSKI A, WIJEYESINGHE S, LEE WY, et al. Neutrophils recirculate through lymph nodes to survey tissues for pathogens[J]. J Neuroimmunol, 2020, 204(9): 2552. [14] STOJANOSKI S, MANEVSKA N, MAKAZLIEVA T, et al. Sentinel lymph node status versus tumor characteristics, neutrophil to lymphocyte ratio, C-reactive protein levels and C-reactive protein to albumin ratio-prognostic factors for primary cutaneus melanoma[J]. Eur J Nucl Med Mol Imaging, 2019, 46(Supp1): S200. [15] XU NZ, JIAN YB, WANG YX, et al. Evaluation of neutrophil-to-lymphocyte ratio and calcitonin concentration for predicting lymph node metastasis and distant metastasis in patients with medullary thyroid cancer[J]. Mol Clin Oncol, 2018, 9(6): 629. -

 点击查看大图
点击查看大图
图(3)表(4)
计量
- 文章访问数: 3544
- HTML全文浏览量: 1999
- PDF下载量: 13
- 被引次数: 0
