

-
前列腺癌(PCa)是老年男性常见恶性肿瘤之一,发病率在男性恶性肿瘤排名第2位,死亡率位列第5位。PCa在全世界各地的发病率相差超过25倍,在澳大利亚、新西兰、北美、欧洲等国家最高,在亚洲最低[1]。虽然PCa在中国的发病率低于西方国家[2],但是近年来由于饮食结构的改变,社会老龄化,以及生活水平和医疗诊断水平的提高,中国PCa的发病率显著提高[3]。2020年中国PCa发病率约15.6/10万,新确诊病例超过11万,死亡病例超过一万[4]。由于PCa症状比较隐蔽,获得诊断的病人大多已处于晚期或并发多处转移。因此早期发现并诊断PCa显得尤为重要,早期的PCa病人经过系统治疗,往往可以取得良好的效果[5]。目前对于PCa的筛查主要有直肠指检和前列腺特异性抗原(PSA)检测,PSA检测联合直肠指检可以提高局限性PCa的早期诊断率和治愈率[6]。其中PSA作为PCa特异性的标志物,已经成为PCa的一线筛查手段[7]。为了解我市60岁以上老年男性PSA水平以及分布情况,探究PSA筛查与PCa早期诊断与治疗之间的联系,选取2020年5-7月在扬州大学附属医院体检的60岁以上老年男性3 102名,完整地记录PSA筛查结果并进行详细分析。现作报道。
-
选取体检的60岁以上老年男性3 102名,具有完整随访信息。排除标准: (1)确诊PCa;(2)近期做过前列腺直肠指检;(3)近期患有前列腺炎(近期有尿路刺激征或排尿异常症状,经抗炎治疗后好转);(4)患有严重心、肝等内脏疾病;(5)其他由于各种原因不能配合调查者。平均年龄(71.87±5.15)岁;PSA平均(2.18±3.03)ng/mL,PSA < 4 ng/mL 2 719(87.65%)例,PSA 4~10 ng/mL 305(9.83%)例,PSA>10 ng/mL者78(2.51%)例。根据中华医学会老年人年龄划分标准,将人群分为60~岁组,70~岁组和80~岁组。
-
体检者均上午空腹来体检中心,抽取肘静脉血3 mL,抽血前1周未行前列腺按摩和直肠指检等检查。血标本经处理后离心分离血清。检测仪器为雅培i2000型全自动化学发光免疫分析仪,检测方法为化学发光免疫分析法,试剂为配套试剂,仪器操作由专门人员严格按照标准化操作规程进行。对PSA异常(≥4 ng/mL)的老年人,凡是符合前列腺穿刺指征并排除禁忌证者, 在B超引导下经会阴用细针穿刺前列腺组织。采取12点穿刺法,在传统6点的基础上增加左、右叶外侧底部、中部、尖部各一点,用甲醛溶液固定标本并送病理检查,明确是否为PCa并进行Gleason评分。前列腺穿刺指征: (1)直肠指检发现结节;(2)PSA>10 ng/mL;(3)PSA水平为4~10 ng/mL,fPSA/tPSA或PASD值异常或B超发现前列腺低回声结节或MRI发现异常信号。前列腺穿刺禁忌证: (1)凝血功能障碍;(2)免疫功能低下,糖尿病病人血糖未控制;(3)急性前列腺炎,会阴部皮肤破溃、真菌性皮炎等皮肤感染。
-
采用方差分析、q检验、χ2检验及秩和检验。
-
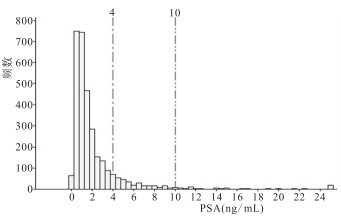
3 102名老年男性PSA值集中于0~2 ng/mL;当4≤PSA < 10 ng/mL时,PSA值越大,出现的频数越小;当PSA>10 ng/mL时,出现的频数较小且无规律性,频数在PSA≥24 ng/mL区间略有回升(见图 1)。随着年龄的增加,每个年龄组的研究对象对应的PSA平均水平呈上升趋势,满足方程Y=0.041 27X-0.820 1,R2=0.457 8,P < 0.01;血清PSA正常人群的PSA平均值随着年龄的增加也呈上升趋势,满足方程Y=0.023 53X+0.240 6(X>60),R2=0.192 3,P < 0.05;对于PSA异常的对象,PSA的平均水平与年龄线性关系无意义(P>0.05)(见表 1)。血清PSA与年龄满足Y=0.041 44X-0.799 2(X>60),R2=0.005,P < 0.01。PSA正常的对象中,随着年龄增大, PSA呈升高趋势,满足Y=0.012 48X+0.438 2(X>60),R2=0.005 2,P < 0.01。对于PSA异常的对象,其PSA水平与年龄的线性关系无意义(见表 2)。

图 1 体检老年男性PSA分布直方图
自变量 因变量 拟合线性归回方程 R2 P 年龄 所有PSA平均值 Y=0.041 27X-0.820 1(X>60) 0.475 8 < 0.01 年龄 正常PSA平均值 Y=0.023 53X+0.240 6(X>60) 0.192 3 < 0.05 年龄 异常PSA平均值 Y=0.016 11X+6.9460(X>60) 0.003 6 >0.05 表 1 所有PSA、正常PSA、异常PSA平均值与年龄构建线性回归方程
自变量 因变量 拟合线性归回方程 R2 P 年龄 所有PSA Y=0.041 44X-0.799 2(X>60) 0.005 0 < 0.01 年龄 正常PSA Y=0.012 48X+0.438 2(X>60) 0.005 2 < 0.01 年龄 异常PSA Y=-0.012 20X+9.0730(X>60) 0.000 1 >0.05 表 2 所有PSA、正常PSA、异常PSA与年龄构建线性回归方程
单因素方差分析显示,PSA在3组间差异有统计学意义(P < 0.01),其中70~岁组、80~岁组PSA均高于60~岁组(P < 0.05)(见表 3)。通过分析发现,随着年龄的增加,PSA水平异常的比例明显增高(P < 0.01)(见表 4)。共有62名老年人接受了前列腺穿刺活检,其中PSA在4~10 ng/mL 38人,穿刺诊断为癌14人(36.8%);PSA>10 ng/mL 24人,穿刺诊断为癌15人(62.5%)。随着PSA水平的升高,前列腺穿刺阳性的比例升高,差异有统计学意义(χ2=3.89,P < 0.05)(见表 5)。对穿刺阳性对象的肿瘤分期发现,随着PSA的升高,肿瘤的Gleason评分越高,危险系数越大,差异具有统计学意义(uc=2.55,P < 0.05)(见表 6)。
分组 n PSA F P MS组内 60~岁 1 418 1.95±2.81 70~岁 1 464 2.35±3.20* 7.94 < 0.01 9.167 80~岁 220 2.54±3.16* q检验: 与60~岁组比较*P < 0.05 表 3 各年龄组PSA水平比较(x±s;ng/mL)
分组 n PSA < 4 ng/mL PSA≥4 ng/mL χ2 P 60~岁 1 418 127 9(90.20) 139(9.80) 70~岁 1 464 126 1(86.14) 203(13.86) 19.65 < 0.01 80~岁 220 179(81.36) 41(18.64) 表 4 研究对象年龄与PSA水平之间的关系[n; 百分率(%)]
PSA/(ng/mL) n PCa 良性 χ2 P 4~10 38 14(36.84) 24(63.16) 3.89 < 0.05 >10 24 15(62.50) 9(37.50) 表 5 穿刺诊断为癌与PSA水平之间的关系[n; 百分率(%)]
PSA/(ng/mL) n Gleason评分 uc P 6分 7分 8分 9分 4~10 14 10(71.4) 4(28.6) 0(0.0) 0(0.0) 2.55 < 0.05 >10 15 4(26.7) 8(53.3) 1(6.7) 2(13.3) 表 6 PSA水平与穿刺阳性肿瘤Gleason评分之间的关系[n; 百分率(%)]
-
研究[8]显示,随着年龄的增加,PSA水平异常的比例明显增高。本研究中,PSA≥4 ng/mL 139人, 随着年龄的增加,PSA水平异常的比例明显增高。分析其中的原因,PSA主要由前列腺上皮细胞合成分泌[9],富集于人类的前列腺腺泡及导管上皮细胞细胞质[10]。随着人年龄的增加,前列腺腺体往往处于一种增生的状态,此时储存分泌的PSA增加。此外,高龄也是PCa的一个重要危险因素[11]。PCa时前列腺上皮细胞增殖失去调控,正常的腺管组织遭到破坏, PSA由淋巴系统进入血液循环,导致血清PSA出现巨大波动[4]。因此随着年龄的增大,PSA异常的可能性越大。本研究中PSA≥4 ng/mL者383人,其中有62人同意进行经B超引导下前列腺组织穿刺活检。其中4~10 ng/mL 38人,穿刺诊断为癌者14人,Gleason评分6分者10人,7分者4人。PSA>10 ng/mL有24人,穿刺诊断为癌者15人,其中Gleason评分6分者有4人,7分者8人,8分者1人,9分者2人。笔者发现在PSA 4~10 ng/mL这个区间内穿刺阳性率较低36.8%,其中大多数为前列腺良性病变,与CAGLAYAN等[12]研究结果一致。而当PSA>10 ng/mL时,穿刺阳性率较高,其患癌的风险远高于PSA 4~10 ng/mL者。本次研究中我们还发现PSA与肿瘤的Gleason评分相关,随着PSA的升高,肿瘤的Gleason评分越高,危险系数越大。亦有研究[13-14]发现PSA同前列腺肿瘤的分期与Gleason评分有相关性,其研究结果证明了高PSA与Gleason在7分以上或更高级别PCa病人的高死亡率有相关性。因此,合理的PSA筛查有助于PCa的早期诊断与治疗[15],对于PSA处于>10 ng/mL的高区间的老年男性应给予重点关注,合理的前列腺穿刺活检对于早期诊断,改善PCa就诊即晚期的现有局面有重大意义[16]。在本次研究中我们还对年龄和PSA数据进行相关性分析,发现在所有研究对象中,PSA水平与年龄呈正相关。在PSA < 4 ng/mL的研究对象中,随着年龄的增大,PSA随之升高,PSA水平与年龄也呈正相关[17],猜测由于在低PSA水平时前列腺良性及恶性病变罹患率较低,研究对象主要为健康人群,PSA水平主要由年龄决定。而在PSA≥4 ng/mL的研究对象中,年龄与PSA水平失去规律性的联系,一方面考虑可能是样本数量不够;另一方面猜测,随着PSA水平升高老年男性PCa及前列腺良性病变的患病率增加[18],而这些病变的产生与遗传、代谢、年龄、种族等都有着很大联系[19]。良性前列腺增生时PSA水平与前列腺体积呈正相关[20],在PCa时,组织恶变的分级越高,危险系数越大,PSA水平越高。此时年龄只是PSA水平一种影响因素[21],PSA主要由是否患病及其严重程度决定。
本次研究中进行前列腺穿刺的共有62人,穿刺结果为PCa的共有29人,部分病人在我院或者其他医院进行了PCa根治术,术后恢复良好。在我院接受PCa根治术者共13人,13例病人的临床分期均未出现远处转移,3例4 ng/mL < PSA < 10 ng/mL的病人分期为局限性,在PSA在>10 ng/mL这个区间内的病人有7例病人临床分期为局限性,3例病人为局部转移。PSA筛查提示了罹患早期PCa的潜在风险[22],早期的诊断与治疗延长了病人的生存时间以及提高了病人的生活质量[23]。血清PSA检验技术应用于临床后,提高了PCa的临床诊断率,为PCa病人获得早期治疗创造了可能。PSA与年龄、种族、体质量指数等多种因素有关[24]。国内外研究人员开发出一系列PSA衍生指标以及其他诊断方法(如MRI、超声、直肠指检结果和其他肿瘤标志物)联合应用能够进一步提高PCa的早期诊断准确率[11, 24-25],我们要灵活选取各个指标,全面地对每个病人进行评估,合理穿刺活检,提高PCa病人早期诊断率。
综上,随着年龄的增大,PSA异常的可能性越大。当PSA处于高区间(>10 ng/mL)时,其患癌的风险远远高于低区间。随着PSA的升高,肿瘤的Gleason评分越高,危险系数越大。进行PSA筛查有助于PCa的早期诊断与治疗。本次研究还存在的一些不足之处,如穿刺活检对象均为PSA异常者,下一步我们将PSA < 4 ng/mL但其他相关检查怀疑PCa的病人纳入穿刺;并且本研究主要选取了扬州地区60岁以上健康体检的老年男性PSA的数据,样本量稍显不足,且样本起点年龄偏高,下一步我们将适当降低筛查年龄,并扩大筛查人数进行研究。
以PSA筛查为基础前列腺癌早期诊断与治疗的研究
Early diagnosis and treatment of prostate cancer based on PSA screening
-
摘要:
目的了解扬州地区60岁以上老年男性前列腺特异性抗原(PSA)水平, 探讨PSA筛查与前列腺癌早期诊断与治疗之间的联系。 方法制定详细的入选与排除标准, 选取扬州地区2020年5-7月体检的60岁以上老年男性3 102例, 均具有完整随访信息。采用化学发光酶免疫分析法检测体检者血清PSA水平, 对符合前列腺癌穿刺标准者, 进行B超引导下经会阴前列腺组织穿刺活检并进行Gleason评分。 结果随着年龄的增加, PSA水平异常的比例明显增高(P < 0.01)。共有62名老年人接受了前列腺穿刺活检, 其中PSA在4~10 ng/mL 38人, 穿刺诊断为癌14人(36.8%); PSA>10 ng/mL 24人, 穿刺诊断为癌15个(62.5%)。随着PSA水平的升高, 前列腺穿刺阳性的比例升高(P < 0.05)。对穿刺阳性对象的肿瘤分期发现, 随着PSA的升高, 肿瘤的Gleason评分越高, 危险系数越大(P < 0.05)。 结论随年龄增加, PSA呈现上升趋势, 且PSA水平升高, 前列腺癌的发生可能性越大, 恶性程度也随之增加。对于老年男性建议进行早期、定期PSA检查。 Abstract:ObjectiveTo investigate the level of prostate specific antigen (PSA) in elderly men over 60 years old in Yangzhou, and explore the relationship between PSA screening and early diagnosis and treatment of prostate cancer. MethodsThe detailed inclusion and exclusion criteria was formulated, and 3 102 elderly men over 60 years old who underwent physical examination in Yangzhou from May to July 2020 with complete follow-up information were selected.The serum PSA level was detected by chemiluminescent enzyme immunoassay.The patients who met the prostate cancer puncture criteria were subjected to transperineal prostate biopsy guided by B-ultrasound, and Gleason score was performed. ResultsWith the increase of age, the proportion of abnormal PSA level increased significantly (P < 0.01).A total of 62 elderly patients underwent prostate biopsy, of which 38 patients had PSA between 4-10 ng/mL, and 14 patients (36.8%) were diagnosed as cancer; PSA>10 ng/mL in 24 cases, and 15 (62.5%) cases were diagnosed as cancer by puncture.With the increase of PSA level, the proportion of positive prostate puncture increased (P < 0.05).According to the tumor staging of puncture positive subjects, with the increase of PSA, the higher the Gleason score of tumor and the greater the risk coefficient (P < 0.05). ConclusionsWith the increase of age, PSA shows an upward trend, and the higher the level of PSA, the greater the possibility of prostate cancer, and the higher the degree of malignancy.Early and regular PSA examination is recommended for elderly men. -
Key words:
- prostate neoplasms /
- prostate-specific antigen
-
表 1 所有PSA、正常PSA、异常PSA平均值与年龄构建线性回归方程
自变量 因变量 拟合线性归回方程 R2 P 年龄 所有PSA平均值 Y=0.041 27X-0.820 1(X>60) 0.475 8 < 0.01 年龄 正常PSA平均值 Y=0.023 53X+0.240 6(X>60) 0.192 3 < 0.05 年龄 异常PSA平均值 Y=0.016 11X+6.9460(X>60) 0.003 6 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 所有PSA、正常PSA、异常PSA与年龄构建线性回归方程
自变量 因变量 拟合线性归回方程 R2 P 年龄 所有PSA Y=0.041 44X-0.799 2(X>60) 0.005 0 < 0.01 年龄 正常PSA Y=0.012 48X+0.438 2(X>60) 0.005 2 < 0.01 年龄 异常PSA Y=-0.012 20X+9.0730(X>60) 0.000 1 >0.05
下载: 导出CSV
表 3 各年龄组PSA水平比较(x±s;ng/mL)
分组 n PSA F P MS组内 60~岁 1 418 1.95±2.81 70~岁 1 464 2.35±3.20* 7.94 < 0.01 9.167 80~岁 220 2.54±3.16* q检验: 与60~岁组比较*P < 0.05
下载: 导出CSV
表 4 研究对象年龄与PSA水平之间的关系[n; 百分率(%)]
分组 n PSA < 4 ng/mL PSA≥4 ng/mL χ2 P 60~岁 1 418 127 9(90.20) 139(9.80) 70~岁 1 464 126 1(86.14) 203(13.86) 19.65 < 0.01 80~岁 220 179(81.36) 41(18.64)
下载: 导出CSV
表 5 穿刺诊断为癌与PSA水平之间的关系[n; 百分率(%)]
PSA/(ng/mL) n PCa 良性 χ2 P 4~10 38 14(36.84) 24(63.16) 3.89 < 0.05 >10 24 15(62.50) 9(37.50)
下载: 导出CSV
表 6 PSA水平与穿刺阳性肿瘤Gleason评分之间的关系[n; 百分率(%)]
PSA/(ng/mL) n Gleason评分 uc P 6分 7分 8分 9分 4~10 14 10(71.4) 4(28.6) 0(0.0) 0(0.0) 2.55 < 0.05 >10 15 4(26.7) 8(53.3) 1(6.7) 2(13.3)
下载: 导出CSV
-
[1] CULP MB, SOERJOMATARAM I, EFSTATHIOU JA, et al. Recent global patterns in prostate cancer incidence and mortality rates[J]. Eur Urol, 2020, 77(1): 38. doi: 10.1016/j.eururo.2019.08.005 [2] 王茹月, 叶雨. PSA衍生指标诊断前列腺癌的研究进展[J]. 中华男科学杂志, 2019, 25(7): 655. doi: 10.13263/j.cnki.nja.2019.07.015 [3] 杨进益, 杨明州, 魏伟, 等. 前列腺癌发生发展的流行病学研究进展[J]. 临床泌尿外科杂志, 2017, 32(9): 721. doi: 10.13201/j.issn.1001-1420.2017.09.018 [4] 前列腺癌筛查中国专家共识(2021年版)[J]. 中国癌症杂志, 2021, 31(5): 435. [5] ZHU Y, MO M, WEI Y, et al. Epidemiology and genomics of prostate cancer in Asian men[J]. Nat Rev Urol, 2021, 18(5): 282. doi: 10.1038/s41585-021-00442-8 [6] TCHIR D, FARAG M, SZAFRON M. Prostate-specific antigen (PSA) screening rates and factors associated with screening in Eastern Canadian men: Findings from cross-sectional survey data[J]. Can Urol Assoc J, 2020, 14(7): E319. [7] CATALONA WJ. Prostate cancer screening[J]. Med Clin North Am, 2018, 102(2): 199. doi: 10.1016/j.mcna.2017.11.001 [8] DE LIMA MM, FILHO SSJ, TOBIAS-MACHADO M. Association between PSA and age in Macuxi ethnic population of the Brazilian Amazon forest region[J]. Res Rep Urol, 2018(10): 159. [9] 张红双, 李杨亮, 陆佳. 急性前列腺炎患者血清前列腺特异性抗原的变化及其意义[J]. 蚌埠医学院学报, 2014, 39(5): 627. doi: 10.13898/j.cnki.issn.1000-2200.2014.05.045 [10] BAI X, JIANG Y, ZHANG X, et al. The Value of prostate-specific antigen-related indexes and imaging screening in the diagnosis of prostate cancer[J]. Cancer Manag Res, 2020, 12: 6821. doi: 10.2147/CMAR.S257769 [11] 朱刚, 张凯. 中国前列腺癌筛查的现状和挑战[J]. 山东大学学报(医学版), 2019, 57(1): 11. [12] CAGLAYAN V, ONEN E, AVCI S, et al. Lymphocyte-to-monocyte ratio is a valuable marker to predict prostate cancer in patients with prostate specific antigen between 4 and 10 ng/dl[J]. Arch Ital Urol Androl, 2019, 90(4): 270. doi: 10.4081/aiua.2018.4.270 [13] TEMEL MC, EDIZ C, AKAN S, et al. Association of Gleason score with PSA values and serum testosterone levels measured prior to prostate biopsy[J]. J Coll Physicians Surg Pak, 2020, 30(4): 399. doi: 10.29271/jcpsp.2020.04.399 [14] WANG J, ABUDUREXITI M, SHAO N, et al. The U shape of prostate-specific antigen and prostate cancer-specific mortality in high-grade metastatic prostate adenocarcinoma[J]. Eur Urol Focus, 2020, 6(1): 53. doi: 10.1016/j.euf.2018.08.024 [15] 燕小朋, 张学珍, 梁姗. 经直肠超声引导下前列腺穿刺活检结合血清PSA早期诊断前列腺癌价值[J]. 蚌埠医学院学报, 2018, 43(5): 637. [16] 余宗泽, 韩德军, 吴强. 前列腺特异性抗原4~10μg/L患者前列腺癌检出率及与年龄和病理分级的相关性分析[J]. 肿瘤预防与治疗, 2019, 32(6): 533. doi: 10.3969/j.issn.1674-0904.2019.06.011 [17] PAZETO CL, LIMA TFN, TRUZZI JC, et al. PSA kinetics before 40 years of age[J]. Int Braz J Urol, 2018, 44(6): 1114. doi: 10.1590/s1677-5538.ibju.2017.0710 [18] HE T, MULLINS CD. Age-related racial disparities in prostate cancer patients: a systematic review[J]. Ethn Health, 2017, 22(2): 184. [19] TR R. Prostate cancer genetics: variation by race, ethnicity, and geography[J]. Semin Radiat Oncol, 2017, 27(1): 3. [20] 黄考平, 温世和, 杨天. 血清PSA与良性前列腺增生临床病理的相关性研究[J]. 中国实用医药, 2019, 14(34): 66. [21] 朱旋, 张忠民, 胡少炜, 等. 中老年男性非前列腺癌住院患者血清PSA及其相关指标的特点分析[J]. 现代泌尿生殖肿瘤杂志, 2018, 10(2): 98. [22] 魏利军, 刘海, 吴永珍, 等. 綦江区前列腺癌健康筛查的临床意义[J]. 蚌埠医学院学报, 2016, 41(9): 1144. [23] PINSKY PF, PROROK PC, YU K, et al. Extended mortality results for prostate cancer screening in the PLCO trial with median follow-up of 15 years[J]. Cancer, 2017, 123(4): 592. [24] DALL'ERA MA, DEVERE-WHITE R, RODRIGUEZ D, et al. Changing incidence of metastatic prostate cancer by race and age, 1988-2015[J]. Eur Urol Focus, 2019, 5(6): 1014. [25] 郭振毅. F-PSA、VEGF和IGF-P水平联合检测在前列腺癌中的临床意义[J]. 数理医药学杂志, 2021, 34(5): 680. -

 点击查看大图
点击查看大图
图(1)表(6)
计量
- 文章访问数: 2782
- HTML全文浏览量: 1546
- PDF下载量: 18
- 被引次数: 0
