

-
急性胰腺炎(acute pancreatitis, AP)是一种迅速发作的胰腺炎症,可导致轻微到严重的、甚至危及生命的状况;由于多种病因(胆道疾病、胰管阻塞、酗酒、暴饮暴食、感染、手术、药物等)引起的胰腺及其周围组织被胰腺分泌的消化酶自身消化所产生的急性化学性炎症,使胰腺发生水肿、出血甚至坏死的一种炎症反应[1-2]。鉴于AP的临床症状(急性腹痛、按压痛、反跳痛等)与急腹症难以鉴别区分,且AP发病凶险,病死率高(20%~30%)的特点[3],因此,早期做出明确诊断就显得尤为重要。本研究收集了我院2017年7月至2021年3月70例收治的AP病人,采用干化学法检测血清脂肪酶(LPS)、淀粉酶(AMS)及C反应蛋白(CRP)水平,探讨它们在AP诊断中的价值。现作报道。
-
70例AP病人,其中男47例,女23例,年龄12~94岁。同期收治的非胰腺炎病人30例,男16例,女14例,其中急性阑尾炎2例,胆囊炎9例,急性腹膜炎11例,急性胃肠炎2例,肠梗阻6例。
-
采集病人静脉血2~3 mL于无抗凝剂的真空采血管中,待血液完全凝固析出血清后,3 000 r/min离心5 min,分离血清。使用强生干化学分析仪(VITROS 5600)检测血清LPS、AMS及CRP水平;试剂为厂家配套,所有试剂均在有效期内,试剂的质控和定标均符合要求。以血清LPS>300 U/L、AMS>125 U/L、CRP>10 mg/L作为阳性判断标准。
-
采用t(或t′)检验、χ2检验和ROC曲线。
-
AP组病人血清LPS、AMS阳性检出率分别为78.57%和77.14%,明显高于非AP组阳性检出率。而2组CRP差异无统计学意义(P>0.05)(见表 1)。
分组 n LPS阳性率 AMS阳性率 CRP阳性率 AP组 70 78.57(55/70) 77.14(54/70) 81.43(57/70) 非AP组 30 23.33(7/30) 13.33(4/30) 70.00(21/30) χ2 — 27.20 35.10 1.60 P — < 0.01 < 0.01 >0.05 表 1 2组血清LPS、AMS及CRP的阳性率比较(%)
-
70例AP组的血清LPS、AMS及CRP水平均高于非AP组(P < 0.01)(见表 2)。
分组 n LPS/(U/L) AMS/(U/L) CRP/(mg/L) AP组 70 1135.8±105.4 525.4±63.8 62.43±4.9 非AP组 30 204.4±23.9 86.7±7.9 18.3±0.4 t — 69.86* 56.53* 74.77* P — < 0.01 < 0.01 < 0.01 *示t′值 表 2 2组血清LPS、AMS及CRP水平比较(x±s)
-
两项指标联合检测的灵敏度和特异性较单项检测都有不同程度的增高,当AMS、LPS、CRP三项指标联合检测时,其诊断的灵敏度达到95.7%,特异度为98.0%,联合检测在诊断AP价值最大(见表 3)。
指标 AMS LPS CRP AMS+LPS AMS+CRP LPS+CRP AMS+LPS+CRP 灵敏度 77.14 78.57 81.43 90.04 88.66 91.46 95.75 特异度 75.50 73.60 38.82 96.76 88.91 85.60 98.04 表 3 AMS、LPS、CRP水平及联合检测在AP诊断上的灵敏度和特异度(%)
-
通过ROC曲线分析发现,在AP的诊断上LPS、AMS准确性明显高于CRP,其中LPS的曲线下面积(AUC)最大,为0.823;其次为AMS的0.785,LPS略微优于AMS,三者联合检测的AUC为0.844,说明LPS、AMS在AP的诊断和检测上要明显优于CRP(见图 1、表 4)。
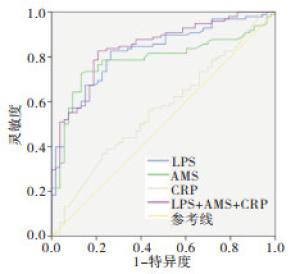
图 1 血清LPS、A MS和CRP水平在AP诊断中的ROC曲线
指标 AUC(95%CI) P 约登指数 cut-off值 LPS 0.823(0.756~0.890) < 0.01 0.562 183.5 AMS 0.785(0.710~0.860) < 0.01 0.592 115.5 CRP 0.564(0.470~0.659) >0.05 0.142 72.88 联合 0.844(0.780~0.907) < 0.01 0.619 — 表 4 AMS、LPS、CRP水平诊断AP效能的比较
-
AP是临床常见的一种迅速发作的胰腺炎症,病人常表现为腹痛、腹胀、恶心、呕吐、发热、黄疸以及器官多功能障碍[4]。一般初期表现较轻,但容易被忽视而转变为重症AP,此时病人较为痛苦,且病死率较高。因此,早期做出明确诊断就能为病人的治疗和预后带来十分重要的作用。
目前,AP的诊断基于两个标准:(1)具有典型腹部疼痛的AP的临床症状;(2)血清AMS和LPS的值超过正常水平3倍或更高以及影像学检测结果。在AP发生时,血清AMS在症状出现后5~8 h就升高,24 h达到高峰,在3~4 d恢复正常,虽然AMS的升高程度与胰腺损伤程度无关,但是其升高程度越高,则发生AP的可能性就越大;然而,也有一些重症胰腺炎病人会出现AMS不增高的现象[5]。同时AMS在其他组织中也可以分泌,如部分肠道梗阻及胆管疾病病人也可出现增高[6]。血清LPS是胰腺组织分泌的一种特有的消化酶,在AP发作后4~8 h升高,24 h达到高峰,8~14 d恢复正常,半衰期为6.9~13.7 h,且LPS基本不受其他因素影响,可以作为AP发作的一个良好指标[7-8]。研究显示,在AP的诊断中,血清AMS的敏感性为63.6%,LPS为99.5%,而特异性方面,无明显差别,分别为99.4%和99.2%[9]。CRP是一种急性时相反应蛋白,反映机体是否处于急性期的指标,目前已被临床广泛应用于疾病的诊断和治疗过程中。CRP水平在AP的发生、发展过程中表现为逐步上升的趋势,这对于判断胰腺细胞损坏程度具有良好判断价值[10-11],但是CRP在AP的诊断方面缺少特异性,因为CRP在很多炎症反应中都可增高。
本研究结果显示,AP组的血清AMS、LPS水平均明显高于对照组(P < 0.05)。两项指标联合检测的灵敏度和特异度较单项检测都有不同程度的增高,且当AMS、LPS、CRP三项指标联合检测时,其诊断AP的灵敏度达到95.7%,特异度为98.0%,都明显增高。从ROC曲线下面积可以看出,在对AP的诊断上,LPS、AMS灵敏度明显高于CRP,其中LPS的AUC为0.823,最大,其次为AMS的0.785,说明LPS、AMS在AP的诊断上优于CRP。通过联合检测血清LPS、AMS和CRP,发现AP诊断的灵敏度和特异度都有很大的提高。可见,这三项指标可作为临床诊断AP、严重程度的判断以及疗效观察等的很好的参考指标。这与李溪等[12]采用联合检测AMS、LPS及CRP诊断AP的研究结果相似。吴松等[13]研究也发现联合检测AMS、LPS对诊断AP具有较高敏感度与特异度,并能够对AP临床治疗效果及预后具有很好预测效果。但也有报道[14]显示,在诊断AP方面,血清LPS比AMS具有更高的敏感度,且LPS增高持续时间长,因此建议仅检测LPS,不必要增加病人的负担和检测的支出,但本研究显示,联合检测价值更高。
综上所述,血清AMS、LPS及CRP在AP病人都出现增高现象,联合三项检测可以提高AP的诊断效率,具有很好的临床应用价值。
血清脂肪酶、淀粉酶及C反应蛋白联合检测对急性胰腺炎诊断的意义
Significance of combined determination of serum lipase, amylase and C-reactive protein in the diagnosis of acute pancreatitis
-
摘要:
目的探讨血清脂肪酶(LPS)、淀粉酶(AMS)及C反应蛋白(CRP)对急性胰腺炎(AP)临床诊断的意义。 方法采用强生干化学分析仪(VITROS 5600)检测70例AP和30例非AP病人的血清LPS、AMS及CRP水平,对2组数据进行比较分析。 结果AP组血清LPS、AMS及CRP水平均高于非AP组(P < 0.01),两项指标联合检测的灵敏度和特异度较单项检测都有不同程度的增高,当AMS、LPS、CRP三项指标联合检测时,其诊断的灵敏度达到95.7%,特异度为98.0%,ROC曲线中血清LPS、AMS曲线下面积较高。 结论血清LPS、AMS及CRP三项联合检测可以有效提高AP的诊断效果,具有很好的临床应用价值。 Abstract:ObjectiveTo explore the significance of lipase(LPS), amylase(AMS) and C-reactive protein(CRP) in the diagnosis of acute pancreatitis(AP). MethodsThe levels of peripheral blood LPS, AMS and CRP in 70 AP patients and 30 non-AP patients were detected using dry chemical analyzer(VITROS 5600), and the data in two groups were analyzed. ResultsThe serum levels of LPS, AMS and CRP in AP group were higher than those in control group(P < 0.01).The sensitivity and specificity of the combined detection of the two indicators were higher than that of the single detection.When the three indicators of AMS, LPS and CRP were combined, the diagnostic sensitivity and specificity of which reached 95.7% and 98.0%, and the area under the ROC curve of serum LPS and AMS was relatively high. ConclusionsThe combined detection of serum LPS, AMS and CRP can effectively improve the diagnostic effects of AP, and which is worthy of clinical application. -
Key words:
- acute panereatitis /
- amylase /
- lipase /
- C-reactive protein
-
表 1 2组血清LPS、AMS及CRP的阳性率比较(%)
分组 n LPS阳性率 AMS阳性率 CRP阳性率 AP组 70 78.57(55/70) 77.14(54/70) 81.43(57/70) 非AP组 30 23.33(7/30) 13.33(4/30) 70.00(21/30) χ2 — 27.20 35.10 1.60 P — < 0.01 < 0.01 >0.05  下载: 导出CSV
下载: 导出CSV
表 2 2组血清LPS、AMS及CRP水平比较(x±s)
分组 n LPS/(U/L) AMS/(U/L) CRP/(mg/L) AP组 70 1135.8±105.4 525.4±63.8 62.43±4.9 非AP组 30 204.4±23.9 86.7±7.9 18.3±0.4 t — 69.86* 56.53* 74.77* P — < 0.01 < 0.01 < 0.01 *示t′值
下载: 导出CSV
表 3 AMS、LPS、CRP水平及联合检测在AP诊断上的灵敏度和特异度(%)
指标 AMS LPS CRP AMS+LPS AMS+CRP LPS+CRP AMS+LPS+CRP 灵敏度 77.14 78.57 81.43 90.04 88.66 91.46 95.75 特异度 75.50 73.60 38.82 96.76 88.91 85.60 98.04
下载: 导出CSV
表 4 AMS、LPS、CRP水平诊断AP效能的比较
指标 AUC(95%CI) P 约登指数 cut-off值 LPS 0.823(0.756~0.890) < 0.01 0.562 183.5 AMS 0.785(0.710~0.860) < 0.01 0.592 115.5 CRP 0.564(0.470~0.659) >0.05 0.142 72.88 联合 0.844(0.780~0.907) < 0.01 0.619 —
下载: 导出CSV
-
[1] LIPPI G, VALENTINO M, CERVELLIN G. Laboratory diagnosisi of acute pancreatitis: in search of the holy grail[J]. Crit Rev Clin Lab Sci, 2012, 49(1): 18. doi: 10.3109/10408363.2012.658354 [2] BROWN TT, PRAHLOW JA. Postmortem serum amylase and lipase analysis in the diagnosis of acute pancreatitis[J]. Acad Forensic Pathol, 2018, 8(2): 311. doi: 10.1177/1925362118782071 [3] TOMESCU D, POPESCU MH, DAVID C, et al. Clinical effects of hemoadsorption with CytoSorb in patients with severe acute pancreatitis: A case series[J]. Int J Artif Organs, 2019, 42(4): 190. doi: 10.1177/0391398818823762 [4] ROMPIANESI G, HANN A, KOMOLAFE O, et al. Serum amylase and lipase and urinary trypsinogen and amylase for diagnosis of acute pancreatitis[J]. Cochrane Daeabase Syst Rev, 2017, 4(4): CD012010. [5] WANG YY, QIAN ZY, JIN WW, et al. Acute pancreatitis with abdominal bloating and distension, normal lipase and amylase: a case report[J]. Medicine(Baltimore), 2019, 98(15): e15138. [6] INOUE H, UEMURA S, HARADA K, et al. Risk factors for acute pancreatitis inpatients with accidental hypothermia[J]. Am J Emerg Med, 2019, 37(2): 189. doi: 10.1016/j.ajem.2018.05.008 [7] 姚丽娜, 顾建文, 史伟峰. 淀粉酶、脂肪酶联检对提高急性胰腺炎诊断的临床价值分析[J/CD]. 临床医药文献电子杂志, 2017, 4(97): 19031. doi: 10.3877/j.issn.2095-8242.2017.97.010 [8] ZHANG Y, YE X, DENG T, et al. Serum amylase as a biomarker for early prediction and diagnosis of post-endoscopic retrograde cholangiopancreatography pancreatitis[J]. Ir J Med Sci, 2020, 189(1): 163. doi: 10.1007/s11845-019-02089-2 [9] CHANG JWY, CHUNG CH. Diagnosing acute pancreatitis: amylase or lipase?[J]. Hong kong J Emerg Med, 2011, 18: 20. doi: 10.1177/102490791101800104 [10] 许楠. 生化检测指标在急性胰腺炎诊断中的临床价值[J]. 中国当代医药, 2018, 25(30): 125. doi: 10.3969/j.issn.1674-4721.2018.30.041 [11] STIRLING AD, MORAN NR, KELLY ME, et al. The predictive value of C-reactive protein(CRP) in acute pancreatitis-is interval change in CRP an additional indicator severity?[J]. HPB(Oxford), 2017, 19(10): 874. [12] 李溪, 周迎春. 血清淀粉酶、C反应蛋白、白细胞联合检测对急性胰腺炎鉴别的价值研究[J]. 检验医学与临床, 2019, 16(2): 161. doi: 10.3969/j.issn.1672-9455.2019.02.005 [13] 吴松, 李治君, 沈钢. 血淀粉酶等联合检测在急性胰腺炎诊断及预后评估中的价值[J]. 热带医学杂志, 2018, 18(5): 621. doi: 10.3969/j.issn.1672-3619.2018.05.016 [14] ISMAIL OZ, BHAYANA V. Lipase or amylase for the diagnosis of acute pancreatitis[J]. Clin Biochem, 2017, 50(18): 1275. doi: 10.1016/j.clinbiochem.2017.07.003 -

 点击查看大图
点击查看大图
图(1)表(4)
计量
- 文章访问数: 3955
- HTML全文浏览量: 1703
- PDF下载量: 9
- 被引次数: 0
