



-
动脉瘤出血破入脑室病人预后较差,病人较早出现高颅压及低灌注,同时血凝块降解产物迅速进入脑脊液循环引起继发损害,并且动脉瘤还有再破裂危险,所以该类病人死亡率及病残率较高。早期进行外引流并注入溶栓剂是临床处理脑室出血较常见的方法,及时对破裂动脉瘤进行栓塞也是挽救病人生命的必要措施[1]。在治疗过程中借助颅内压监测装置实时监测颅压,可以为制定和调整治疗策略提高依据。本研究分析了23例动脉瘤出血破入脑室病人的临床特点、诊断、处理与结果,旨在探讨动脉瘤破裂出血破入脑室病人应用颅内压监测装置的可行性。现作报道。
-
选择2010年6月至2016年6月我科共收治的23例出血破入脑室病人作为研究对象,所有病人头颅CT提示脑室出血,伴有蛛网膜下腔出血;经CTA或DSA确诊为动脉瘤,动脉瘤位于前循环19例,后循环4例。本组病人男8例,女15例;年龄28~69岁。HUNT-HESS分级:Ⅱ级2例,Ⅲ级12例,Ⅳ级9例。
-
23例病人中19例病人入院后即行全脑血管造影,发现颅内动脉瘤破裂出血,遂行动脉瘤栓塞术,予以致密填塞。栓塞术后即刻放置颅内压监测装置(脑室型,带引流功能,美国强生公司)。4例病人入院后即放置颅内压监测装置,72 h内予以动脉瘤栓塞(见图 1~4)。穿刺点为右侧冠状缝前及中线旁各2 cm,穿刺方向为脑室额角,深度5 cm,穿刺成功有血性脑脊液流出时,抬高引流管,读取初始压力。颅内压监测装置放置后保持引流通畅,血凝块堵塞致引流管不畅时,经引流管往脑室内注射尿激酶使得引流管通畅。病人咳嗽、躁动、吸痰时,颅内压短时内急剧升高,会流出大量脑脊液,故引流管放于较高的位置,保持管内脑脊液搏动,一般在穿刺点上10~20 cm,前3天控制每日引流量100~200 mL,后期控制每日引流量200~300 mL。
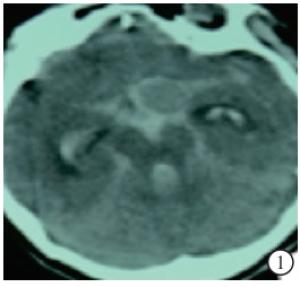
图 1 病人入院时头颅CT平扫,可见前循环巨大动脉瘤

图 2 置入颅内压监测装置后头颅CT平扫

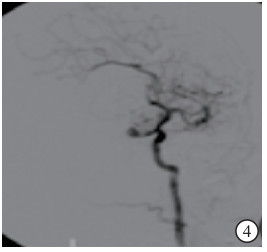
图 3 栓塞前造影
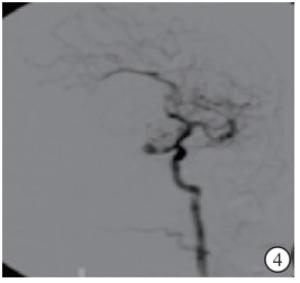
图 4 栓塞后造影。
-
每小时记录一次颅内压值。主要目的是早期发现动脉瘤再出血,及时处理颅高压。控制血管收缩压160 mmHg以下。目标颅内压控制在25 mmHg以下。颅内压过高时适当增大甘露醇用量,同时增加外引流量,头部抬高30°~45°。部分病人同时使用亚低温疗法后颅内压维持于较低水平。如果颅内压持续过高,立即查头颅CT,排除动脉瘤再破裂、脑梗死的发生。
-
每天进行脑脊液细胞学检查和生化检查,每3 d做一次脑脊液细菌培养,拔除导管时做导管末端细菌培养。每天监测体温变化。脑脊液有核细胞数高,糖、氯化物低,体温高,常提示中枢神经系统感染,需加强抗感染治疗。
-
病人预后采用格拉斯哥结局评分(GOS):5分, 痊愈良好,恢复正常生活;4分, 中度残疾,但尚可独立生活,可以在保护下工作;3分, 严重残疾,日常生活不能独立,需要照顾;2分, 长期持续的植物生存状态;1分, 死亡。
-
采用方差分析和q检验。
-
本组病人初始颅内压平均28.52 mmHg,HUNT-HESS分级3组间初始颅内压差异无统计学意义(P>0.05)(见表 1)。
分组 n 初始颅内压/mmHg GOS评分/分 HUNT-HESS Ⅱ级 2 22.50±7.78 5.00±0.01 HUNT-HESS Ⅲ级 12 29.33±7.34 3.33±0.98* HUNT-HESS Ⅳ级 9 28.78±8.50 2.44±0.88**# F — 0.61 7.86 P — >0.05 <0.01 MS组内 — 64.314 0.810 q检验:与HUNT-HESS Ⅱ级比较*P<0.05,**P<0.01;与HUNT-HESS Ⅲ级比较#P<0.05 表 1 各组初始颅内压和出院时GOS评分
-
共有3例病人发生颅内感染,根据脑脊液培养及药敏试验结果予以抗生素治疗。1例为女性,45岁,入院时HUNT-HESS Ⅲ级,后抗炎治疗有效,出院时GOS 3分。1例为男性,57岁,入院时HUNT-HESS Ⅳ级,后死亡。1例为女性,43岁,入院时HUNT-HESS Ⅳ级,后抗炎治疗有效,出院时GOS 2分。
-
共有2例病人发生动脉瘤破裂再出血。1例为男性,58岁,入院时HUNT-HESS Ⅲ级,后死亡。1例为女性,28岁,入院时HUNT-HESS Ⅳ级,出院时GOS 2分。
-
颅内压装置放置时间3~12 d,平均6.87 d。发生颅内感染的病人放置时间较长,平均9.67 d。
-
共有4例病人术后发生脑积水,占本组存活21例病人的19.05%。所有脑积水病人均成功予以脑室腹腔分流术。
-
HUNT-HESS分级各级间GOS评分差异有统计学意义(P<0.01),HUNT-HESS分级评分越高,GOS评分越低(P<0.05~P<0.01)(见表 1)。
-
颅内压监护在动脉瘤破裂出血病人中的使用目前没有权威性指南[2]。脑室出血可能引起急性梗阻性脑积水,应用带有引流功能的颅内压监测装置,引流的同时可以进行颅内压实时监控,手术简单易行,监护简便、测压准确。
动脉瘤破裂出血病人施行脑室外引流后可能增加了动脉瘤再次破裂出血的机会,但是减少了急性梗阻性脑积水的机会,减轻了高颅压引起的继发脑损害[3]。为了减少再出血的概率,我们控制引流量和引流高度,防止颅压太低。美国心脏与卒中协会建议在条件许可的情况下尽可能早地给予动脉瘤栓塞术[4],该组病人早期均予以动脉瘤致密填塞,进一步减少了动脉瘤再出血的概率。病人最初的神经功能损害多是由高颅压及低灌注引起的[5],颅压不能太高,我们一般控制在20~25 mmHg,主要通过适当引流血性脑脊液的速度和运用脱水剂治疗。这样可以维持脑灌注压大于50~55 mmHg。在动脉瘤栓塞完成后,由于动脉瘤再破裂的危险明显降低,尽量控制颅内压在20 mmHg以下。在这一过程中颅内压监护装置为临床决策提供数据支持,起到非常重要的作用。
在应对早期病人出血颅内压高的情况时,有些学者采取了去骨瓣减压术[6]。去骨瓣减压能迅速有效地降低颅内压,增加脑灌注,降低死亡率,但是是否能改善预后仍存在争议。本组病人在监测颅压的同时,适当引流脑脊液,达到部分减压效果,能维持颅压于一个合理的水平,同时考虑到手术可能的并发症与风险以及经济成本,未进行去骨瓣减压。
颅内压监测装置植入病人发生颅内感染的概率并不是很高,FLIBOTTE等[7]报道211例颅内压监测装置植入病人17例发生颅内感染(8.1%),跟病人年龄和装置植入时间长短有关系,颅内感染影响NICU治疗时长和住院时长,但是对病人预后没有明显影响。是否预防性使用抗生素仍有争议,常规使用抗生素会诱发细菌耐药性,同时药物还可能带来潜在的不良反应。我们只在病人有体温高,脑脊液化验白细胞数高的时候应用抗生素,日常注意引流管处的消毒换药,减少头皮逆行感染至颅内的可能性。在怀疑有颅内感染时,马上予以经验用药,同时留置脑脊液细菌培养,一般48 h左右有结果,这时根据药敏结果予以抗生素治疗,同时尽快拔除颅内压监测及其他外引流装置,间断进行腰椎穿刺释放脑脊液并进行脑脊液细胞学检查、生化检查及细菌学检查。通过这些方法能极大减少颅内压植入装置带来的颅内感染危险。
颅内压监测装置在动脉瘤出血破入脑室病人中的应用
Application of the intracranial pressure monitoring device in patients with intracranial aneurysm hemorrhaging into the ventricle
-
摘要:
目的探讨动脉瘤破裂出血破入脑室病人应用颅内压监测装置的可行性。 方法回顾性分析23例动脉瘤出血破入脑室病人的临床特点、并发症及预后。 结果病人根据HUNT-HESS分级分为3组,初始颅内压平均28.52 mmHg。术后有3例病人发生颅内感染,有2例病人发生动脉瘤破裂再出血,有4例病人发生脑积水。颅内压装置放置时间3~12 d,平均6.87 d。出院时HUNT-HESS分级各级的格拉斯哥预后评分为Ⅱ级5.00分,Ⅲ级3.33分,Ⅳ级2.44分,各级间格拉斯哥预后评分差异有统计学意义(P<0.01)。 结论应用颅内压监测装置于动脉瘤破裂出血破入脑室病人,有助于实时监测病人颅内压,治疗过程顺利,病人预后评分较高。 Abstract:ObjectiveTo investigate the feasibility of the application of intracranial pressure monitoring device in patients with intracranial aneurysm hemorrhaging into the ventricle. MethodsThe clinical characteristics, complications and prognosis in 23 patients with intracranial aneurysm hemorrhaging into the ventricle were retrospectively analyzed. ResultsAll patients were divided into three groups according to the HUNT-HESS classification.The average initial intracranial pressure was 28.52 mmHg.Postoperative intracranial infection occurred in 3 cases, the aneurysm rupture rebleeding in 2 cases were identified, and the postoperative hydrocephalus in 4 cases were found.The intracranial pressure device was implanted for 3 to 12 days(mean 6.87 days).At discharge, the GOS scores of grade Ⅱ, Ⅲ and Ⅳ HUNT-HESS were 5.00, 3.33 and 2.44 points, respectively.The differences of GCS scores in different grades were statistically significant(P < 0.01). ConclusionsThe application of intracranial pressure monitoring device in patients with intracranial aneurysm hemorrhaging into the ventricle can help to monitor the intracranial pressure in real-time, and ensure the smooth treatment course and better prognosis. -
Key words:
- aneurysm /
- intraventricular hemorrhage /
- intracranial pressure monitoring
-
表 1 各组初始颅内压和出院时GOS评分
分组 n 初始颅内压/mmHg GOS评分/分 HUNT-HESS Ⅱ级 2 22.50±7.78 5.00±0.01 HUNT-HESS Ⅲ级 12 29.33±7.34 3.33±0.98* HUNT-HESS Ⅳ级 9 28.78±8.50 2.44±0.88**# F — 0.61 7.86 P — >0.05 <0.01 MS组内 — 64.314 0.810 q检验:与HUNT-HESS Ⅱ级比较*P<0.05,**P<0.01;与HUNT-HESS Ⅲ级比较#P<0.05  下载: 导出CSV
下载: 导出CSV
-
[1] DEY M, STADNIK A, AWAD IA.Spontaneous intracerebral and intraventricular hemorrhage:advances in minimally invasive surgery and thrombolytic evacuation, and lessons learned in recent trials[J].Neurosurgery, 2014, 1(2):142. [2] 王翔, 张乔, 毛庆, 等.颅内压监测与脑室外引流在动脉瘤性蛛网膜下腔出血中的应用[J].中华神经外科杂志, 2014, 30(2):137. doi: 10.3760/cma.j.issn.1001-2346.2014.02.011 [3] DELLA PEPA GM, SCERRATI A, ALBANESE A, et al.Protective effect of external ventricular drainage on cerebral vasospasm.A retrospective study on aneurysmal SAH treated endovascularly[J].Clin Neurol Neurosurg, 2014, 124:97. doi: 10.1016/j.clineuro.2014.06.030 [4] MAYBERG MR, BATJER HH, DACEY R, et al.Guidelines for the management of aneurysmal subarachnoid hemorrhage:a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association[J].Stroke, 2012, 43(6):1711. doi: 10.1161/STR.0b013e3182587839 [5] DE OLIVEIRA MANOEL AL, GOFFI A, MAROTTA TR, et al.The critical care management of poor-grade subarachnoid haemorrhage[J].Critical Care, 2016, 20(1):1. [6] JUSSEN D, MARTICORENA S, SANDOW N, et al.Ultra-early decompressive hemicraniectomy in aneurysmal intracerebral hemorrhage:a retrospective observational study[J].Minerva Anestesiol, 2015, 81(4):398. [7] FLIBOTTE JJ, LEE KE, KOROSHETZ WJ, et al.Continuous antibiotic prophylaxis and cerebral spinal fluid infection in patients with intracranial pressure monitors[J].Neurocritical Care, 2004, 1(1):61. doi: 10.1385/NCC:1:1:61 -

 点击查看大图
点击查看大图

图(4)表(1)
计量
- 文章访问数: 3802
- HTML全文浏览量: 1962
- PDF下载量: 11
- 被引次数: 0
