

-
体素内不相干运动磁共振扩散加权成像(IVIM-DWI)能够分离和量化组织内水分子扩散和微循环灌注特征信息,已在临床肿瘤中开展应用,如宫颈、肝脏、直肠、前列腺等[1-4],但对直肠癌组织学类和病理分级相关报道不多见。黏液性腺癌作为直肠腺癌亚型,因富含较多黏液、实质成分较少,更易发生淋巴结转移、静脉侵袭、术后复发和转移,具有预后较差特点[5-6],术中需扩大切除范围、彻底淋巴结清扫等,且其对新辅助放化疗不敏感[7],术前进行组织类型、病理分级的预测至关重要。本研究旨在探讨直肠癌体素内不相干运动(IVIM)参数与组织类型、病理分级间相关性,评价参数鉴别诊断效能,以期帮助术前预测和制定治疗方案。现作报道。
-
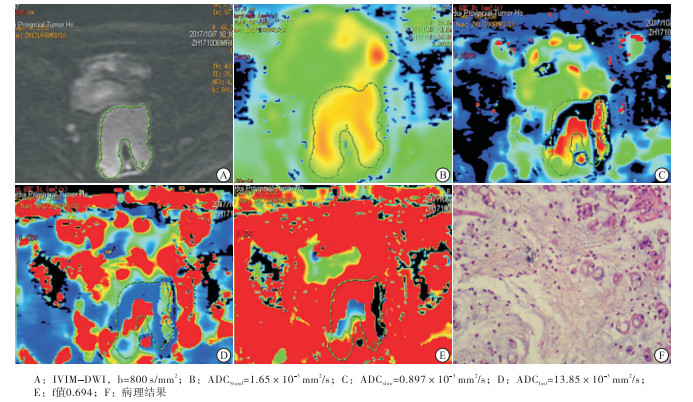
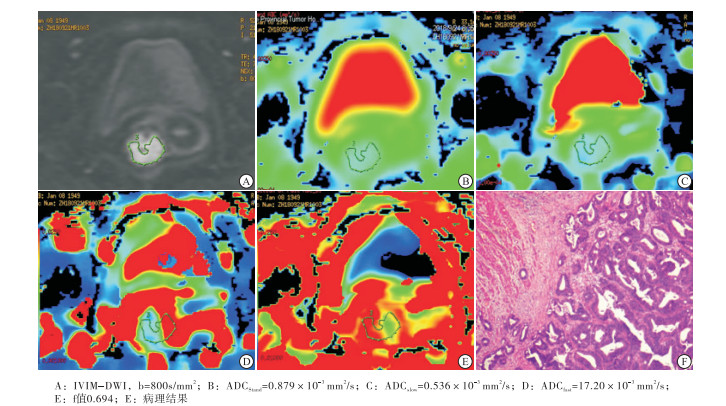
收集2016年7月至2018年11月我院经手术病理证实的直肠普通腺癌29例、黏液性腺癌12例临床资料,术前均接受直肠常规及高分辨MRI、IVIM(10个b值)扩散加权序列扫描。纳入标准:(1)MRI扫描前均经内镜活检确诊的直肠癌病人;(2)MR常规及多b值IVIM序列资料完整,且具有术后病理记录;(3)检查前未接受手术、放化疗等治疗。排除标准:(1)肠镜活检病理结果为腺瘤伴恶变;(2)腺癌病理结果未描述组织分化;(3)图像质量不佳,不便于观察与准确勾画肿瘤边界。其中普通组男21例,女8例;年龄45~84岁;病理分级Ⅱ级20例,Ⅱ~Ⅲ级5例,Ⅳ级4例,典型病例见图 1。黏液组男4例,女8例;年龄47~79岁;3例黏液成分占比25%~50%,典型病例见图 2。2组病人均知情同意并签署知情同意书。

图 1 病人女,69岁,直肠腺癌Ⅱ级

图 2 病人女,79岁,直肠黏液性腺癌
-
采用GE Signa HDxT 3.0T MR扫描仪,8通道Torsor相控阵线圈,中心定位耻骨上缘,常规FSE序列T1WI:TR 540 ms,TE 7.5 ms,NEX 2,矩阵352×192,T2WI压脂:TR 5 000 ms,TE 30 ms,NEX 2,矩阵320×256;层厚6.0 mm,间距2.0 m,FOV 4×24 m,IVIM序列10个b值(0、10、20、50、100、200、400、800、1 200、2 000 s/mm2);TR 4 000 ms,TE 65 ms,矩阵96×130,NEX 6.LAVA-Flex动态增强采用高压注射器肘静脉团注法,对比剂轧喷酸葡胺0.2 mmol/kg, 速率2.0 mL/s,动脉期、静脉期、延时期多期扫描。
-
应用GE ADW4.5后处理工作站,由2名高年资主治医师分别随机对图像进行分析,利用Functool-MADC测量IVIM参数拟合出标准扩散系数(ADC)、真扩散系数(D)、假扩散系数(D*)、灌注分数(f值)伪彩图及参数值;在b值800 s/mm2图像上设置感兴趣区(region of interest, ROL),结合高分辨T2WI、增强T1WI图,避开出血、坏死、水肿区,选取不少于3个层面手动勾画肿块实质区域ROL,取各参数均值并记录。
-
采用t检验、方差分析和受试者工作特征曲线(receiver operationg characteristic curve, ROC)分析。
-
2组标准ADC、D、f值差异具有统计学意义(P < 0.01),D*值差异无统计学意义(P>0.05)(见表 1)。
分组 n 标准ADC/(×10-3 mm2/s) D D* f值/% 普通组 29 0.88±0.11 0.63±0.12 15.65±18.73 34.54±10.82 黏液组 12 1.17±0.22 0.87±0.18 12.48±5.24 48.89±12.97 t — -4.12 -3.0 -0.57 -3.65 P — <0.01 <0.01 >0.05 <0.01 表 1 2组病人IVIM参数比较(x±s)
-
普通组不同病理分级病人间的标准ADC、D、D*、f值差异均无统计学意义(P>0.05)(见表 2)。
病理分级 n 标准ADC/(×10-3 mm2/s) D D* f值/% Ⅱ级 20 0.91±0.08 0.68±0.08 18.89±21.67 31.97±10.14 Ⅱ~Ⅲ级 5 0.87±0.09 0.62±0.06 6.32±1.04 39.46±7.78 Ⅳ级 4 0.82±0.12 0.55±0.10 11.16±7.56 43.48±11.44 F — 0.33 0.70 1.04 2.86 P — >0.05 >0.05 >0.05 >0.05 表 2 普通组不同病理分级间IVIM参数比较(x±s)
-
标准ADC、D、f值鉴别黏液腺癌和普通腺癌的ROC曲线下面积(AUC)依次为0.748、0.814、0.758(P < 0.05);ROC曲线评价标准ADC、D、f值鉴别诊断的阈值、敏感性、特异性依次为0.998×10-3mm2/s、88.3%、55.7%,0.81×10-3mm2/s、91.7%、72.9%,43.05%、75.0%、72.9%,D值具有最佳诊断效能(见图 3)。
-
传统的单指数模型DWI成像,ADC值包含组织扩散和灌注双重信息,高b值可间接反映组织扩散特征[8],对量化分析具有局限性。IVIM序列采用多b值双指数模型描述体素内微观运动,理论基础是自旋回波信号对分子运动的敏感性,假设组织内微循环是一种非一致性随机运动,血液受磁化矢量的影响发生相位位移而导致信号衰减[9]。并采用双指数拟合、通过非线性最小二乘法得出参数,即标准ADC值,反映组织内扩散和灌注综合信息;D值代表纯水分子真性扩散;D*值与微血管灌注相关假扩散,受血流速度、微血管形态影响;f值反映微循环灌注在组织总扩散中容积比;IVIM序列可分离体素内扩散、灌注相关信息特征,可对组织内信息定量分析,术前可对直肠癌组织学类型、病理分级判断提供帮助。
标准ADC反映组织综合信息[8],而D值主要受细胞结构、密集度和核质比等因素影响[10]。本研究结果显示,普通腺癌标准ADC、D值明显低于黏液性腺癌,与崔兰兰等[11-12]研究结果一致。提示普通腺癌ADC、D值与细胞数目、密度、排列及核浆比例有关。黏液性腺癌因细胞外大量黏液伴黏液湖,癌细胞含量少,成岛状或小巢状漂浮在黏液湖中,排列疏松伴间质血管稀少。普通腺癌扩散峰度系数K值明显高于黏液性腺癌,与其易缺血坏死、纤维组织增生等异质性较大有关。本研究采用ROC曲线评价参数诊断效能发现,D值诊断与鉴别诊断效能较高,与标准ADC及f值(AUC:0.814和0.748、0.758,P < 0.05)相比具有较高敏感性、特异性,最佳诊断阈值为0.81×10-3 mm2/s,说明组织内水分子扩散较之灌注能更好地反映微环境病理生理特征。
D*值反映毛细血管内血流扩散信息,与平均毛细血管长度、微血管密度、血液流速呈相关关系[10, 13]。理论上肿瘤恶性度高,供血动脉增粗、新生血管生成,微循环灌注增加。程楠等[1]研究显示,宫颈癌D*值高于正常宫颈。但本研究结果显示,普通腺癌与黏液性腺癌间D*值差异无统计学意义,与杨严伟等[14]研究结果一致。其可能原因为恶性肿瘤新生血管不规则、易发出血、瘤栓导致灌注减低;同时也与D*值测量稳定性、可重复性较差相关。研究[15]表明,D*值受多种因素影响,如ROL设置与勾画方法、b值选择、肿瘤异质性、血供、噪声、算法等。
f值反映DWI中D*值所占比例,本研究中,普通腺癌f值明显低于黏液性腺癌,与文献[1, 14]结论一致,提示恶性肿瘤微血管丰富且不规则、间质内压力增高,存在微观小囊变和坏死、纤维组织等。WILLIAMS等[16]发现恶性肿瘤伴随血管内皮生长因子异常表达,诱导新生不成熟血管生成、通透性高易破碎,更加重缺血、氧和坏死等,导致灌注相应减低。因此认为血管内皮生长因子并不一定能代表肿瘤真实血供,评价肿瘤微循环血流及血容量,需结合病理相关指标研究证实。其是否与黏液性腺癌异质性小、结构疏松,网状间质血管受影响较少,f值在复杂扩散形式中占比相对增加有关,尚有待深入研究。
恶性肿瘤病理分级、分化关乎其预后,韩帅等[3]研究显示,直肠癌D值与细胞分化呈正相关关系,与病理分级呈负相关关系。文献[13, 17]显示,标准ADC、D值可用于部分恶性肿瘤病理分级评估。本研究结果显示,标准ADC、D、D*、f值在普通腺癌不同病理分级间差异均无统计学意义,与既往结论不同,可能与既往研究病理分级仅选择对高、低级别比较有关,而本组采用Ⅱ级20例、Ⅱ~Ⅲ级5例、Ⅳ级4例进行比较,也可能与Ⅱ~Ⅲ级和Ⅳ级数据较少有关,有待大样本量进一步分析。
本研究局限性在于:本组病理分级没有Ⅰ级高分化腺癌,以Ⅱ级分化为主,Ⅱ~Ⅲ级、Ⅳ级普通腺癌和黏液性腺癌样本量较少;3例黏液性腺癌中黏液成分不足50%,可能导致结果偏倚,需增加样本量进一步研究。总之,不同组织类型直肠癌IVIM参数不同,可作为无创鉴别普通腺癌、黏液性腺癌有效方法之一,D值能够真实反映肿瘤微环境水分子扩散信息特征,且诊断效能较高,可为术前直肠癌组织类型预测、治疗方案选择提供帮助。
体素内不相干运动参数与直肠癌组织类型和病理分级的相关性研究
Study on the correlation between inteavoxel incoherent motion parameters and histologic type and pathological grade of rectal cancer
-
摘要:
目的探讨体素内不相干运动(IVIM)参数与直肠癌组织学类型、病理分级的相关性。 方法收集经病理证实的直肠普通腺癌29例(普通组)和黏液性腺癌12例(黏液组),术前行常规MR及10个b值(0、10、20、50、100、200、400、800、1 200、2 000 s/mm2)IVIM序列扫描,比较2组肿瘤实质区标准扩散系数(ADC)、真扩散系数(D)、假扩散系数(D*)、灌注分数(f值),采用受试者工作特征曲线(ROC)评价各参数诊断效能。 结果普通组标准ADC、D、f值均明显低于黏液性腺癌(P < 0.01)。普通组不同病理分级病人间标准ADC、D、D*、f值差异均无统计学意义(P>0.05)。ROC曲线分析显示,标准ADC、D、f值鉴别诊断普通腺癌和黏液性腺癌的阈值、敏感性、特异性及ROC曲线下面积依次为0.998×10-3 mm2/s、88.3%、55.7%、0.748,0.81×10-3mm2/s、91.7%、72.9%、0.814,43.00%、75.0%、72.9%、0.758。 结论IVIM参数能定量反映不同组织学类型直肠癌细胞密集度及灌注特征,其中以D值诊断与鉴别价值最佳,有助于术前预测和治疗方案制定。 -
关键词:
- 直肠肿瘤 /
- 体素内不相干运动参数 /
- 体素内不相干运动磁共振扩散加权成像
Abstract:ObjectiveTo explore the correlation between inteavoxel incoherent motion(IVIM) parameters and histologic type and pathological grade of rectal cancer. MethodsTwenty-nine patients with common adenocarcinoma of rectum and 12 patients with mucinous adenocarcinoma diagnosed by pathology were divided into the common group and mucinous group, respectively.Two groups were detected using routine MR and IVIM scan(b=0, 10, 20, 50, 100, 200, 400, 800, 1 200, 2 000 s/mm2) before operation.The apparent diffusion coefficient(ADC), true diffusion coefficient(D), pseudo-diffusion coefficient(D*) and perfusion score(f value) were compared between two groups.The diagnostic efficiency of parameters were evaluated using receiver operating characteristic curve(ROC). ResultsThe ADC, D and f value in common group were significantly lower than that in mucinous group(P < 0.01).The differences of the ADC, D and f value in different pathology grades patients in common group were not statistically significant(P>0.05).The results of ROC analysis showed that the optimal threshold value, sensitivity, specificity and area under the curve ROL in common adenocarcinoma of rectum patients and mucinous adenocarcinoma diagnosed by the ADC, D and f value were 0.998×103 mm2/s, 88.3%, 55.7%, 0.748, 0.81×10-3 mm2/s, 91.7%, 72.9%, 0.814, 43.0%, 75.0%, 72.9% and 0.758, respectively. ConclusionsIVIM parameter can quantitatively reflect the characteristics of cell density and perfusion of different histological types of rectal cancer.The D value has the highest diagnostic efficiency, which is helpful for preoperative prediction and making of clinical treatment plans. -
表 1 2组病人IVIM参数比较(x±s)
分组 n 标准ADC/(×10-3 mm2/s) D D* f值/% 普通组 29 0.88±0.11 0.63±0.12 15.65±18.73 34.54±10.82 黏液组 12 1.17±0.22 0.87±0.18 12.48±5.24 48.89±12.97 t — -4.12 -3.0 -0.57 -3.65 P — <0.01 <0.01 >0.05 <0.01  下载: 导出CSV
下载: 导出CSV
表 2 普通组不同病理分级间IVIM参数比较(x±s)
病理分级 n 标准ADC/(×10-3 mm2/s) D D* f值/% Ⅱ级 20 0.91±0.08 0.68±0.08 18.89±21.67 31.97±10.14 Ⅱ~Ⅲ级 5 0.87±0.09 0.62±0.06 6.32±1.04 39.46±7.78 Ⅳ级 4 0.82±0.12 0.55±0.10 11.16±7.56 43.48±11.44 F — 0.33 0.70 1.04 2.86 P — >0.05 >0.05 >0.05 >0.05
下载: 导出CSV
-
[1] 程楠, 吕星海.IVIM多模型参数分析对宫颈癌的诊断价值[J].放射学实践, 2017, 32(2):157. [2] ZHU L, CHENG Q, LUO W, et al.A comparative study of apparent diffusion coefficient and intravoxel incoherent motion-derived parameters for the characterization of common solid hepatic tumors[J]. Acta Radiol, 2015, 56(12):1411. doi: 10.1177/0284185114559426 [3] 韩帅, 王立峰, 邵楠楠, 等.体素内不一致运动序列评估直肠癌术前病理分级的可行性研究[J].临床放射学杂志, 2015, 34(12):1929. [4] 温茹, 赵文露, 魏超刚, 等.动态增强MRI和扩散加权定量参数直方图与前列腺癌Gleason评分相关性[J].中华放射学杂志, 2017, 51(5):355. doi: 10.3760/cma.j.issn.1005-1201.2017.05.007 [5] CHAND M, YU S, SWIFT RL, et al.Mucinous carcinoma of the rectum:a distinct clinicopathological entity[J]. Tech Coloproctol, 2014, 18(4):335. [6] NITSCHE U, ZIMMERMANN A, SPÄTH C, et al.Mucinous and signet-ring cell colorectal cancers differ from classical adenocaicionmas in tumor biology and prognosis[J]. Ann Surg, 2013, 258(5):775. doi: 10.1097/SLA.0b013e3182a69f7e [7] MCCAWLEY N, CLANCY C, O'NEILL BD, et al.Mucinous rectal adenocarcinoma is associated with a poor response to neoad-juvant chemoradiotherapy:A systematic review and Meta-analysis[J]. Dis Colon Rectum, 2016, 59(12):1200. doi: 10.1097/DCR.0000000000000635 [8] ⅡMA M, LE BIHAN D.Clinical inteavoxel incoherent motion and diffusion MR imaging:past, present and future[J]. Radiology, 2016, 278(1):13. [9] LE BIHAN D, BRETON E, LALLEMAND D, et al.MR imaging of inteavoxel incoherent motion:application to diffusion and perfusion in neurologic disorders[J]. Radiology, 1986, 161(2):401. doi: 10.1148/radiology.161.2.3763909 [10] NOUGARET S, VARGAS HA, LAKHMAN Y, et al.Intravoxel incoherent motion-derived Histogram metrics for assessment of response sfter combined chemotherapy and radiation therapy in rectal cancer:Initial experience and comparison between singlesection and volumetric analyses[J]. Radiology, 2016, 280(2):446. doi: 10.1148/radiol.2016150702 [11] 崔兰兰, 浦竟, 王玉斌, 等.PET/CT SUV值、WB-DWI ADC值与结直肠癌病理分型的相关性研究[J].中国肛肠病杂志, 2017, 37(8):11. doi: 10.3969/j.issn.1000-1174.2017.08.003 [12] 文子强, 杨心悦, 陈琰, 等.磁共振扩散峰度成像在直肠癌组织学类型及病理分级中的应用[J/CD].消化肿瘤杂志:电子版, 2018, 10(1):11. [13] SHEN N, ZHAO L, JIANG J, et al.Intravoxel incoherent motion diffusion-weighted imaging analysis of diffusion and microperfusion in grsding gliomas and comparision with arterial spin labeling for evaluation of tumor perfusion[J]. J Magn Reson Imaging, 2016, 44(3):620. [14] 杨严伟, 顾晓燕, 陈光强, 等.3.0T磁共振IVIM参数与直肠中分化腺癌T分期相关性初步研究[J].实用放射学杂志, 2016, 32(7):1052. doi: 10.3969/j.issn.1002-1671.2016.07.015 [15] 孟闫凯, 张红梅, 欧阳汉, 等.直肠癌体素内不相干运动参数测量的可重复性研究[J].中华肿瘤杂志, 2017, 39(12):910. doi: 10.3760/cma.j.issn.0253-3766.2017.12.006 [16] WILLIAMS E, MARTIN S, MOSS R, et al.Co-expression of VEGF and CA9 in ovarian high-grade serous carcinoma and relationshap to survival[J]. Virchows Arch, 2012, 461(1):33. doi: 10.1007/s00428-012-1252-9 [17] ZHU Q, YE J, ZHU W, et al.Value of intravoxel incohcrent motion in assessment of pathological grade of clear cell renal cell carcinoma[J]. Acta Radiol, 2018, 59(1):121. doi: 10.1177/0284185117716702 -

 点击查看大图
点击查看大图
图(2)表(2)
计量
- 文章访问数: 3688
- HTML全文浏览量: 2099
- PDF下载量: 7
- 被引次数: 0
