

-
目前临床上治疗进展期胃癌的主要手术方式为胃癌根治术,随着临床上该手术方法的不断发展,学者们逐渐关注如何制定更加安全有效的淋巴结清扫范围来提高病人的预后恢复效果[1]。第三版的胃癌治疗指南给出了明确的胃癌淋巴结清扫(D2)范围,然而肝总动脉后(No.8p)﹑胆总管旁(No.12b)﹑门静脉旁(No.12p)等淋巴结均不在其中[2]。有一项回顾性研究[3]结果显示,773例行局部胃癌D2根治术的病人,术后No.8p、No.12b、No.12p淋巴结的转移率分别为16.44%、7.01%及8.50%,其中发生No.8p淋巴结转移的风险最大。临床上是否可以采取D2+转移率较高的淋巴结清扫,进一步提高病人的远期生存率仍然存在争议[4]。因此本研究对我院2012年2月至2017年6月收治的106例胃癌病人进行随访,探讨进展期胃癌病人术后No.8p淋巴结转移率及其影响因素,并进一步分析No.8p淋巴结转移对胃癌病人远期生存的影响,为临床上提高进展期胃癌病人治疗效果提供科学依据。
-
选取2012年2月至2017年6月我院收治的106例胃癌病人作为本次研究的对象,其中男50例,女56例,年龄(64.9±9.9)岁。病例纳入标准:(1)经病理学检查确诊为进展期胃癌的病人(癌组织已侵入病人胃壁肌层、浆膜层,不论病灶大小,或有无转移,均称为进展期胃癌);(2)经胃癌根治术治疗并进行D2以上淋巴结清扫的病人(均包括No.8p);(3)临床和随访资料完整的病人。排除标准: (1)诊断为早期胃癌的病人;(2)接受新辅助化疗的病人;(3)经姑息性手术治疗的病人。
-
所有病人均接受胃癌根治性手术治疗,切除的范围包括原病灶的切除及规范淋巴结清扫(D2淋巴结清扫术),在此基础上加No.8p淋巴结清扫,远端胃切除行残胃空肠Braun吻合式重建,全胃切除行P襻空肠食管重建。胃癌病人的TNM分期根据美国癌症联合会制定的最新版胃癌分期标准[5]。所有手术均由同一组医生完成。病人在手术前均签署了知情同意书,且本研究也通过了相关机构的伦理审查。
-
本次研究主要评估胃癌根治术病人术后No.8p淋巴结的转移及病人预后情况,在病人出院后2年内每3~6月复查一次,2~5年内每6~12个月复查一次,当病人超过5年以上时,每年对其进行复查,主要随访病人的生存情况、常规化验检查、肿瘤标志物水平及其他辅助检查。截至2019年4月,共随访病人98例(92.45%),随访时间为22~86个月(中位时间为43个月),失访8例(7.55%)。
-
采用χ2检验、多因素logistic分析、log-rank检验和多因素Cox回归分析。
-
发生No.8p淋巴结转移的胃癌病人在年龄、性别、吸烟、体质量指数(BMI)及饮酒等特征上差异均无统计学意义(P>0.05),且肿瘤切除部位、血清白蛋白及血红蛋白含量差异亦均无统计学意义(P>0.05),但肿瘤大小≥4 cm、TNM分期较高以及存在联合脏器切除、术中输血的胃癌病人发生No.8p淋巴结转移的概率较高(P < 0.05)(见表 1)。
因素 n 8p淋巴结转移[n; 百分率(%)] χ2 P 年龄/岁 < 65 54 5(9.26) 1.50 >0.05 ≥65 52 9(17.31) 性别 男 50 6(12.00) 0.12 >0.05 女 56 8(14.29) 吸烟 否 54 5(9.26) 1.50 >0.05 是 52 9(17.31) 饮酒 否 48 8(16.67) 0.92 >0.05 是 58 6(10.34) BMI/(kg/m2) < 18.5 8 1(12.50) 0.14 >0.05 18.5~23.9 42 5(11.90) 24.0~27.9 34 5(14.71) ≥28.0 22 3(13.64) 肿瘤切除部位 近端 51 6(11.76) 2.73 >0.05 远端 45 5(11.11) 全胃 10 3(30.00) 肿瘤大小/cm < 4 32 1(3.12) 4.07 < 0.05 ≥4 74 13(17.57) TNM分期 Ⅰ 5 0(0.00) 9.40 < 0.05 Ⅱ 38 1(2.63) Ⅲ 44 3(6.82) Ⅳ 20 5(25.00) 术中输血 无 95 9(9.47) 11.13 < 0.05 有 11 5(45.45) 联合脏器切除 无 86 8(9.30) 6.06 < 0.05 有 20 6(30.00) 血清白蛋白/(g/L) < 35 41 1(25.00) 0.50 >0.05 ≥35 02 13(12.75) 血红蛋白/(g/L) < 100 13 2(15.38) 0.06 >0.05 ≥100 93 12(12.90) 表 1 影响106例胃癌病人No.8p淋巴结转移的单因素分析
-
以是否发生No.8p淋巴结转移为因变量(0=未发生,1=发生),将年龄、性别及单因素分析中有意义的变量纳入多因素分析,筛选方法采用向后LR法,引入变量标准为α入=0.05,从方程模型中剔除标准α出=0.10。结果显示:性别、TNM分期及肿瘤大小是胃癌病人发生No.8p淋巴结转移的独立影响因素(P < 0.05~P < 0.01)(见表 2)。
变量 B SE Waldχ2 P OR 95%CI 性别 0.413 0.092 19.00 < 0.01 1.491 1.248~1.793 TNM分期 0.728 0.357 4.09 < 0.05 3.473 1.057~5.254 肿瘤大小 0.472 0.073 46.01 < 0.01 1.604 1.397~1.835 表 2 106例胃癌病人No.8p淋巴结转移的多因素logistic回归分析
-
106例胃癌根治术病人中,共完整随访98例病人(92.45%),随访时间为22~86个月(中位时间43个月)。将年龄、性别及单因素分析中影响胃癌病人预后的因素(肿瘤切除部位、肿瘤大小、TNM分期、存在联合脏器切除及No.8p淋巴结转移)纳入Cox多因素分析中,结果表明肿瘤大小、TNM分期及No.8p淋巴结转移为影响胃癌病人预后的独立因素(P < 0.01)(见表 3、4)。
因素 n 5年生存[n;百分率(%)] χ2 P 年龄/岁 < 65 51 21(41.17) 0.09 >0.05 ≥65 47 18(38.30) 性别 男 48 19(39.58) 0.01 >0.05 女 50 20(40.00) 吸烟 否 52 17(32.69) 2.33 >0.05 是 46 22(47.83) 饮酒 否 42 18(42.86) 0.29 >0.05 是 56 21(37.50) 肿瘤切除部位 近端 50 13(26.00) 8.16 < 0.05 远端 42 23(54.76) 全胃 6 3(50.00) 肿瘤大小/cm < 4 26 17(65.38) 9.67 < 0.05 ≥4 72 22(30.56) TNM分期 Ⅰ 4 4(100.00) 9.06 < 0.05 Ⅱ 35 16(45.71) Ⅲ 41 15(36.59) Ⅳ 18 4(22.22) 术中输血 无 91 35(38.46) 0.95 >0.05 有 7 4(57.14) 联合脏器切除 无 80 29(36.25) 2.29 >0.05 有 18 10(55.56) No.8p淋巴结转移 无 83 37(44.58) 5.18 < 0.05 有 15 2(13.33) 表 3 影响98例胃癌病人预后的单因素分析
变量 B SE Waldχ2 P HR 95%CI 肿瘤大小 0.144 0.043 10.67 < 0.01 1.151 1.056~1.241 TNM分期 0.967 0.168 34.41 < 0.01 2.643 1.913~3.652 8p淋巴结转移 0.503 0.154 11.65 < 0.01 1.636 1.238~2.184 表 4 胃癌病人预后的多因素Cox回归分析
所随访的人群5年总生存率为39.80%,存在No.8p淋巴结转移及无No.8p淋巴结转移的病人5年生存率分别为13.33%及44.58%,差异具有统计学意义(P < 0.05)(见图 1)。
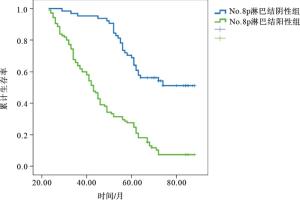
图 1 No.8p淋巴结阳性与阴性进展期胃癌病人生存曲线的比较
-
在对胃癌病人进行手术治疗时,病人的区域淋巴结转移状态是判定其癌症临床分期、术后辅助治疗方案及预后评估的重要依据。然而在目前的临床实践中,并未有一种有效的手段及标准去准确判定胃癌病人区域淋巴结的清扫范围。尤其是在对胃癌病人行D2根治术时,对No.8p淋巴结与No.8a淋巴结的清扫标准不一致,两者之间的分界存在模糊不清的状态[6]。位于肝总动脉周围的第8组淋巴结可分为2组:No.8p与No.8a淋巴结。然而根据第14版日本胃癌“处理规约”,No.8a淋巴结属于进展期胃癌根治术常规淋巴结的清扫范围,但是No.8p淋巴结却不在其中[7]。有研究[8]结果显示,No.8p淋巴结具有较高的转移率及转移度,是否应将其纳入胃癌根治术常规淋巴结清扫范围,需要临床上对No.8p淋巴结转移状态、发生转移的高危因素及其对病人远期预后的影响进行深入的探讨。
本次研究共纳入106例胃癌病人,No.8p淋巴结转移率为13.21%,与同类研究结果[9]相似。陈路川等[7]的研究分析了790例行胃癌根治术的病人,发生No.8p淋巴结转移的病人为93例(11.8%)。李连顺[10]的研究结果显示No.8p淋巴结转移率为11.21%(12/107)。淋巴结转移度逐渐成为临床上研究的热点,可能与其可以准确反映病人疾病分期及预测预后效果有关。LEE等[11]研究发现淋巴结的转移程度可以降低病人的5年生存率,进一步提示要重视No.8p淋巴结转移率及转移程度。通过多因素logistic回归探讨影响胃癌根治术病人No.8p淋巴结转移的高危因素,结果表明,性别、TNM分期较高及肿瘤大小是胃癌根治术病人发生No.8p淋巴结转移的独立危险因素,与同类研究[12]结果一致。在本次研究中,女性的胃癌根治术病人发生No.8p淋巴结转移的风险是男性的1.49倍,与以往研究[7]结论一致。可能原因是由于胃癌为雌激素受体依赖型恶性肿瘤,女性的胃癌组织学恶性程度一般较高,发生转移的可能性增加。同时程元光等[13]的研究并未发现No.8p淋巴结转移与性别之间存在显著相关性,可能与研究的样本量及人群特征不同等因素有关。
同时本研究发现肿瘤较大及TNM分期较高的胃癌根治术病人No.8p淋巴结转移的风险会随之增加,与以往研究结果相似[12, 14]。肿瘤体积较大的病人,其浆膜损伤面积及淋巴管破坏的数目也相应增高,从而进一步增加No.8p淋巴结受累的风险。TNM分期较高的病人,存在其他区域的淋巴结转移,癌细胞在淋巴回流通路中发生进一步转移,从而增加No.8p淋巴结的转移风险[13]。因此,针对TNM分期较高、肿瘤体积较大的No.8p淋巴结转移高危病人,在手术过程中可以合理扩大淋巴结清扫范围,对No.8p淋巴结进行完整及彻底清扫,减少疾病复发及提高病人术后存活率。
目前临床上对No.8p淋巴结清扫的争议主要集中于以下几个方面,首先有学者认为No.8p淋巴结的转移率及转移程度较低,而且该淋巴结的位置处于后腹膜,位置比较深,对其清扫会增加手术时间以及术后并发症的发生风险,最后主要是由于临床上对No.8p淋巴结清扫的临床意义仍不明确,能否可以真正改善病人的预后状况,提高其远期生存率仍存在一定疑虑[8-9]。本研究发现No.8p淋巴结转移的病人5年生存率显著低于未转移组的病人(13.33% vs 44.58%),与其他研究结论一致[3, 15-16],可能原因是由于No.8p淋巴结进入腹主动脉旁淋巴网络的速度较快,当发生转移时,会迅速扩散,影响病人的术后治疗效果。
综之,女性、肿瘤大小≥4 cm及TNM分期较高的行胃癌根治术病人发生No.8p淋巴结转移的风险较大,针对具有上述高危因素的病人,应考虑对No.8p淋巴结进行彻底完整的清扫。合理的清扫No.8p淋巴结还可以进一步增加进展期胃癌病人的远期生存率,建议临床上应有选择的对进展期胃癌病人进行No.8a加No.8p淋巴结清扫。
胃癌病人No.8p淋巴结转移的危险因素及其预后的多因素回归分析
Multivariate regression analysis of the risk factors of No.8p lymph node metastasis and prognosis in patients with gastric cancer
-
摘要:
目的探讨胃癌根治术病人No.8p淋巴结转移的危险因素及其对病人远期预后的影响。 方法对106例行胃癌根治术的病人临床资料进行分析,其中有No.8p淋巴结转移的病人14例,无No.8p淋巴结转移的病人92例,通过多因素logistic回归分析影响病人No.8p淋巴结转移的独立危险因素,Cox回归分析No.8p淋巴结转移对病人远期预后的影响。 结果106例病人中No.8p淋巴结转移率为13.21%。发生No.8p淋巴结转移的胃癌病人在年龄、性别、吸烟、体质量指数及饮酒等特征上差异均无统计学意义(P>0.05),且肿瘤切除部位、血清白蛋白及血红蛋白含量差异亦均无统计学意义(P>0.05),但肿瘤大小≥ 4 cm、TNM分期较高以及存在联合脏器切除、术中输血的胃癌病人发生No.8p淋巴结转移的概率较高(P < 0.05)。多因素logistic回归分析显示,女性、TNM分期、肿瘤大小是胃癌根治术病人发生No.8p淋巴结转移的独立危险因素(P < 0.05~P < 0.01)。完成随访病人共98例(92.45%),随访时间为22~86个月(中位时间43个月),5年生存率为39.80%。No.8p淋巴结转移病人5年生存率为13.33%低于无No.8p淋巴结转移病人的44.58%(P < 0.05)。多因素Cox回归分析结果显示肿瘤大小、TNM分期及No.8p淋巴结转移为影响胃癌根治术病人预后的独立因素(P < 0.01)。 结论性别、TNM分期及肿瘤大小是胃癌病人No.8p淋巴结转移的独立危险因素。 Abstract:ObjectiveTo analyze the risk factors of No.8p lymph metastasis and their effects on long-term prognosis in patients with gastric cancer. MethodsThe clinical data of 106 advanced gastric cancer patients treated with radical operation were analyzed.The patients included 14 cases with No.8p lymph metastasis and 92 cases without No.8p lymph metastasis.The independent risk factors affecting the occurrence of No.8p lymph metastasis were analyzed using multivariate logistic regression analysis, and the effects of No.8p lymph metastasis on the long-term prognosis of patients were analyzed using Cox regression analysis. ResultsThe incidence rate of No.8p lymph metastasis in 106 patients with gastric cancer was 13.21%.Among the patients with No.8p lymph metastasis, there was no statistical significance in the age, gender, smoking, body mass index and drinking(P>0.05), and the differences of the tumor resection site, serum albumin and hemoglobin content were not statistically significant(P>0.05).However, the No.8p lymph metastasis rates in gastric cancer patients with tumor size ≥ 4 cm, higher TNM staging, combined organ resection and intraoperative blood transfusion were higher(P < 0.05).The results of multivariate logistic regression analysis showed that the female, TNM staging and tumor size were the independent risk factors of No.8p lymph metastasis in gastric cancer patients treated with radical operation.A total of 98 patients(92.45%) were followed up for 22 to 86 months(median time for 43 months), and the 5-year survival rate was 39.80%.The 5-year survival rate in patients with No.8p lymph metastasis(13.33%) was lower than that in patients without No.8p lymph metastasis(44.58%)(P < 0.05).The results of multivariate Cox regression analysis showed that tumor size, TNM staging and No.8p lymph metastasis were the independent factors affecting the prognosis of patients(P < 0.01). ConclusionsThe sex, TNM staging and tumor size are the independent risk factors of No.8p lymph metastasis in advanced gastric cancer patients. -
Key words:
- gastric neoplasms /
- lymph /
- metastasis /
- prognosis
-
表 1 影响106例胃癌病人No.8p淋巴结转移的单因素分析
因素 n 8p淋巴结转移[n; 百分率(%)] χ2 P 年龄/岁 < 65 54 5(9.26) 1.50 >0.05 ≥65 52 9(17.31) 性别 男 50 6(12.00) 0.12 >0.05 女 56 8(14.29) 吸烟 否 54 5(9.26) 1.50 >0.05 是 52 9(17.31) 饮酒 否 48 8(16.67) 0.92 >0.05 是 58 6(10.34) BMI/(kg/m2) < 18.5 8 1(12.50) 0.14 >0.05 18.5~23.9 42 5(11.90) 24.0~27.9 34 5(14.71) ≥28.0 22 3(13.64) 肿瘤切除部位 近端 51 6(11.76) 2.73 >0.05 远端 45 5(11.11) 全胃 10 3(30.00) 肿瘤大小/cm < 4 32 1(3.12) 4.07 < 0.05 ≥4 74 13(17.57) TNM分期 Ⅰ 5 0(0.00) 9.40 < 0.05 Ⅱ 38 1(2.63) Ⅲ 44 3(6.82) Ⅳ 20 5(25.00) 术中输血 无 95 9(9.47) 11.13 < 0.05 有 11 5(45.45) 联合脏器切除 无 86 8(9.30) 6.06 < 0.05 有 20 6(30.00) 血清白蛋白/(g/L) < 35 41 1(25.00) 0.50 >0.05 ≥35 02 13(12.75) 血红蛋白/(g/L) < 100 13 2(15.38) 0.06 >0.05 ≥100 93 12(12.90)  下载: 导出CSV
下载: 导出CSV
表 2 106例胃癌病人No.8p淋巴结转移的多因素logistic回归分析
变量 B SE Waldχ2 P OR 95%CI 性别 0.413 0.092 19.00 < 0.01 1.491 1.248~1.793 TNM分期 0.728 0.357 4.09 < 0.05 3.473 1.057~5.254 肿瘤大小 0.472 0.073 46.01 < 0.01 1.604 1.397~1.835
下载: 导出CSV
表 3 影响98例胃癌病人预后的单因素分析
因素 n 5年生存[n;百分率(%)] χ2 P 年龄/岁 < 65 51 21(41.17) 0.09 >0.05 ≥65 47 18(38.30) 性别 男 48 19(39.58) 0.01 >0.05 女 50 20(40.00) 吸烟 否 52 17(32.69) 2.33 >0.05 是 46 22(47.83) 饮酒 否 42 18(42.86) 0.29 >0.05 是 56 21(37.50) 肿瘤切除部位 近端 50 13(26.00) 8.16 < 0.05 远端 42 23(54.76) 全胃 6 3(50.00) 肿瘤大小/cm < 4 26 17(65.38) 9.67 < 0.05 ≥4 72 22(30.56) TNM分期 Ⅰ 4 4(100.00) 9.06 < 0.05 Ⅱ 35 16(45.71) Ⅲ 41 15(36.59) Ⅳ 18 4(22.22) 术中输血 无 91 35(38.46) 0.95 >0.05 有 7 4(57.14) 联合脏器切除 无 80 29(36.25) 2.29 >0.05 有 18 10(55.56) No.8p淋巴结转移 无 83 37(44.58) 5.18 < 0.05 有 15 2(13.33)
下载: 导出CSV
表 4 胃癌病人预后的多因素Cox回归分析
变量 B SE Waldχ2 P HR 95%CI 肿瘤大小 0.144 0.043 10.67 < 0.01 1.151 1.056~1.241 TNM分期 0.967 0.168 34.41 < 0.01 2.643 1.913~3.652 8p淋巴结转移 0.503 0.154 11.65 < 0.01 1.636 1.238~2.184
下载: 导出CSV
-
[1] DEGIULI M, DE MANZONI G, DI LA, et al. Gastric cancer: Current status of lymph node dissection[J]. World J Gastroenterol, 2016, 22(10): 2875. doi: 10.3748/wjg.v22.i10.2875 [2] 郭飞, 马宜传, 张俊祥, 等. 多排螺旋CT术前诊断胃癌淋巴结转移的价值[J]. 蚌埠医学院学报, 2015, 40(10): 1378. [3] 武卫鹏, 邓靖宇, 梁寒, 等. 远端胃癌淋巴结转移规律及临床意义[J]. 中国肿瘤临床, 2015, 42(18): 906. doi: 10.3969/j.issn.1000-8179.2015.18.183 [4] 梁寒. 局部进展期胃癌的合理淋巴结清扫范围[J]. 中华消化外科杂志, 2015, 14(3): 183. doi: 10.3760/cma.j.issn.1673-9752.2015.03.003 [5] 闻静. 不同部位胃癌临床病理特点分析[J]. 蚌埠医学院学报, 2017, 42(9): 1173. [6] 王向征, 赵宗耀, 张会来, 等. 淋巴结清扫范围对进展期胃癌患者预后的影响研究[J]. 癌症进展, 2019, 17(8): 929. [7] 陈路川, 魏晟宏, 叶再生, 等. 进展期胃癌No. 8p淋巴结转移的危险因素及预后分析[J]. 中华胃肠外科杂志, 2017, 20(2): 218. [8] 叶再生, 曾奕, 魏晟宏, 等. 进展期胃癌No. 8p淋巴结清扫的可行性[J]. 中华胃肠外科杂志, 2018, 21(10): 1129. doi: 10.3760/cma.j.issn.1671-0274.2018.10.010 [9] GUO DJ, YANG K, ZHANG WH, et al. Prognostic Value of Metastatic No. 8p LNs in Patients with Gastric Cancer[J]. Gastroenterol Res Pract, 2015, 2015: 937682. [10] 李连顺. 进展期胃癌第8p和第14v组淋巴结清扫和转移危险因素的分析[D]. 兰州: 兰州大学, 2016. [11] LEE SR, KIM HO, SON BH, et al. Prognostic significance of the metastatic lymph node ratio in patients with gastric cancer[J]. World J Surg, 2012, 36(5): 1096. doi: 10.1007/s00268-012-1520-5 [12] 徐岩, 孙哲, 王振宁, 等. 胃癌不同部位淋巴结转移率及其临床意义的研究[J]. 中国普外基础与临床杂志, 2012, 19(1): 16. [13] 程元光, 文刚, 涂从银, 等. 胃癌第8p淋巴结转移的相关因素分析[J]. 安徽医药, 2014, 18(5): 855. doi: 10.3969/j.issn.1009-6469.2014.05.018 [14] HAN KB, JANG YJ, KIM JH. Clinical significance of the pattern of lymph node metastasis depending on the location of gastric cancer[J]. Gastric Cancer, 2011, 11(2): 86. doi: 10.5230/jgc.2011.11.2.86 [15] TANIZAWA Y, TERASHIMA M. Lymph node dissection in the resection of gastric cancer: review of existing evidence[J]. Gastric Cancer, 2010, 13(3): 137. doi: 10.1007/s10120-010-0560-5 [16] 丁波, 李忠, 刘元直, 等. 进展期胃癌根治术中脾门淋巴结清扫的临床意义[J]. 中国普通外科杂志, 2014, 23(1): 133. -

 点击查看大图
点击查看大图

图(1)表(4)
计量
- 文章访问数: 3365
- HTML全文浏览量: 1825
- PDF下载量: 12
- 被引次数: 0
