


-
外伤是导致颈椎骨折最主要的原因,当受到屈曲暴力时极易合并脱位,骨折大部分伴有脊髓损伤,可能造成高位截瘫甚至死亡[1],脱位严重者合并关节绞锁时常给骨折的复位造成困难。对于明确诊断为颈椎骨折伴脱位的病人,入院检查提示生命体征平稳后,常采取激素冲击、颅骨牵引辅助颈椎复位治疗,目的是为了尽快解除脊髓压迫、减轻脊髓损伤的炎症反应。颅骨牵引时常采用颈椎过伸的姿势,以期达到好的复位效果[2],其规范性和正确性直接关系到病人的生命安全及功能恢复[3]。传统的颈椎牵引体位是使病人仰卧位,床头抬高15°~20°,牵引时使用棉被或浴巾等柔软物品垫高病人肩部,颈部后伸20°[4-5]。但临床护理中发现, 肩背部所垫棉被或浴巾等柔软物品质软且容易塌陷、移位,无法达到有效支撑,病人不舒适,夜间睡眠质量差,甚至出现枕后及棘突处压力性损伤,严重影响牵引效果。为解决以上问题,我们自行设计了符合脊柱生理曲度、能给予有效支撑的“颈椎牵引体位垫”,以此辅助颅骨牵引治疗,可有效提高病人牵引过程中舒适度,减少病人痛苦及压力性损伤等并发症的发生。本研究旨在通过在临床行颅骨牵引时将其与传统填充物进行对比,分析二者舒适度及观察指标的差异,探讨颈椎牵引体位垫在临床应用中的优越性。
-
采用简单随机化的方法,选取我院骨科脊柱及创伤病区自2016年1月至2020年2月收治的64例颈椎骨折脱位需行颅骨牵引治疗的病人,年龄19~56岁,男39例,女25例。纳入标准:(1)病人意识清楚,可配合完成牵引及护理工作;(2)影像学均证实诊断明确的颈椎骨折伴脱位需行颅骨牵引的病人;(3)病人及其家属知情并同意参与本次研究。排除标准:(1)既往颈椎手术史;(2)合并颈椎其他疾患,如颈椎畸形等;(3)牵引过程中出现意识不清等无法配合观察者。颅骨牵引术由同一组经验丰富的脊柱外科医生完成。64例病人随机分为观察组和对照组,每组32例。观察组年龄20~56岁,平均(36.1±9.0)岁,男21例,女11例;对照组年龄19~56岁,平均(35.3±8.9)岁,男18例,女14例。2组年龄、性别均具有可比性。
-
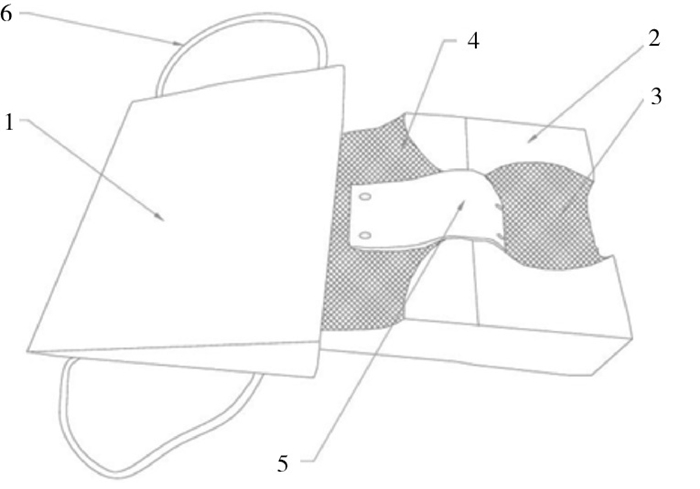
选用加棉、加厚、透气性好的棉布和不易变形的高密度的海绵2块, 分为主体垫和副体垫。主体垫长60 cm,宽50 cm,高16 cm,在垫子上方切割出一深度4 cm、直径20 cm的半圆形头枕槽,符合颈椎生理性前凸设计,内置可拆卸透气棉垫(填充物为烘干黄小米,能够保持颈部高度支撑,有祛湿、按摩功效,透气性好),有效避免了枕部压力性损伤;在上胸段切割出一深度5 cm、直径30 cm的弧形胸部槽,符合胸椎生理性后凸设计,且能提供有效支撑,两旁设有斜形契合肩部的肩部槽。副体垫切割成长60 cm、宽40 cm、高16 cm的三角形斜坡垫,满足腰椎生理性前凸的设计,有效避免腰背棘突处压力性损伤,副体垫两侧设计有拉绳,可以方便操作轴线式翻身,且方便移动病人及日常更换床单(见图 1)。主、副垫中间设计粘扣,增加稳定性,拉链式透气棉布罩可自由拆卸,方便清洗,且一人一垫,避免交叉感染, 该项体位垫已取得专利(专利号:ZL 2019 2 0214671.6)。使用示意图见图 2。
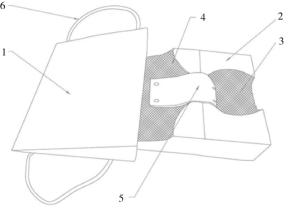
图 1 自制颈椎牵引体位垫示意图(1: 副体垫; 2: 主体垫; 3: 头枕槽; 4: 肩部槽; 5: 胸部槽; 6: 拉绳
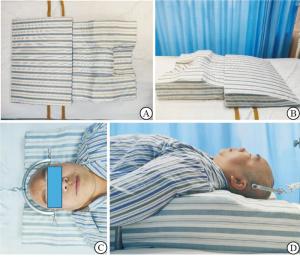
图 2 自制颈椎牵引体位垫使用示意图
-
2组病人均按照颅骨后牵引常规进行护理,予以吸氧、心电监护、禁食水、抗凝等应用,加强心理健康教育及专科护理。2组病人行颅骨牵引时牵引弓均为同一型号牵引弓,行颅骨牵引前均由医生谈知风险并签订同意书,由责任护士告知护理事项并对家属进行相同的培训教育,告知注意事项。对实施护士进行统一培训,并按照统一标准调整自制颈椎牵引体位垫及巾卷的位置及高度。对照组采用颈部以下用巾卷垫高维持过伸姿势,肩背部垫棉被;观察组颈部以下采用自制颈椎牵引体位垫。
-
通过简化McGill量表[6]对病人颈部的疼痛程度进行评估,量表由疼痛分级指数(pain rating index, PRI)、VAS评分及现实疼痛强度评定分数(present pain intensity, PPI)构成,其中PRI由15项组成,其中11个为感觉类,4个为情感类。每个描述语都按照强度等级进行排序:0表示无,1表示轻度,2表示中度,3表示重度。得分越高,表明疼痛带给病人的不良影响越大。PPI和VAS则用以测量疼痛强度。病人行牵引后,于次日、第4天、末次观察时由同一名护士对病人进行指导完成量表的调查。
-
参照2014年EPUAP/NPUAP[7]快速参考指南提出的参考分期标准,收集病人颈部皮肤处发生Ⅰ期压力性损伤的发生例数,各组Ⅰ期压力性损伤发生率等于组内颈部皮肤Ⅰ期压力性损伤发生的病人例数/组内总病例数×100%。
-
使用Likert 7分法[8-9]制定舒适度评分表,由同一名护士对入组对象进行评价指导,牵引过程中第4天评价疼痛程度时指导病人自评颈部舒适度。评分标准:1表示非常不舒服,2表示很不舒服,3表示不舒服,4表示可接受,5表示舒服,6表示舒适度令人放松,7表示非常舒服。评分由1分至7分,分数越高,表示病人在牵引过程中,颈部受支撑的舒适度越好。
-
采用t(或t′)检验、χ2检验和秩和检验。
-
观察组与对照组在牵引次日SF-McGill量表评分差异无统计学意义(P > 0.05),在牵引第4天及末次观察中,观察组的SF-McGill量表评分均低于对照组(P < 0.01)。观察组及对照组在牵引治疗期间压力性损伤发生率为9.4%(3/32)及37.5%(12/32),差异有统计学意义(P < 0.01)(见表 1)。
分组 n SF-McGill量表评分(x±s)/分 Ⅰ期压力性
损伤发生牵引次日 第4天 末次观察 观察组 32 32.0±2.8 25.3±2.7 21.8±1.8 3 对照组 32 32.6±2.6 27.3±1.6 24.1±2.0 12 t — 0.89 3.60* 4.83 7.05# P — > 0.05 < 0.01 < 0.01 < 0.01 *示t′值; #示χ2值 表 1 2组牵引期间SF-McGill量表评分及压力性损伤发生情况
-
在舒适度的观察中,观察组的舒适度评分4(4,5)高于对照组2(2,3),差异有统计学意义(Z=6.51,P < 0.01)。
-
在本研究中,观察组及对照组行牵引治疗时,在第4日及末次观察中,观察组较对照组的SF-McGill量表评分显著降低。即使用自行设计的颈椎牵引体位垫代替传统巾卷填充颈下可减少病人的疼痛程度。病人行颅骨牵引术时需仰卧于病床上,牵引时传统填充使用棉被或浴巾等物品垫高肩背部,单块大都无法达到有效支撑高度,不能持续保持仰卧颈部后伸位体位,无法达到颅骨牵引的要求,可导致牵引时颈部悬空,易导致病人颈肩部疼痛。行多块叠加置于颈下时,虽可达到有效高度,但巾卷不固定、易松散,可能在治疗过程中发生移位。同时,棉被或浴巾等物品其质软或容易塌陷。这些原因均会导致在牵引过程中,病人颈部不能得到有效的支撑,由于牵引重量的存在,病人在牵引过程中颈部肌肉会产生非正常姿势带来的僵硬不适,加剧疼痛感。自制颈椎牵引体位垫在制作中采用高密度的海绵,可提供适当的硬度支撑颈部,不会塌陷;另一方面,整块固定的设计防止牵引过程中发生移位等导致的颈部支撑不良,在研究中,有效减少了病人颈部的疼痛感。同时自制颈椎体位垫在设计中,将脊柱其他部分的生理曲度包含进来,可帮助病人在长期卧床的过程中,保证胸背部及腰背部得到有效的支撑,减少不适感。
-
研究观察中,2组研究对象的Ⅰ期压力性损伤发生有明显的差别,观察组Ⅰ期压力性损伤发生率为9.4%,显著低于对照组的发生率37.5%。压力性损伤发生的原因由压力、剪切力、摩擦力及潮湿导致[10-12],本研究中自制的颈椎牵引体位垫使用了贴合颈部的曲度设计,其在应用过程中,较传统填充使用棉被或浴巾等物品垫高肩部时,有效支撑面积更大且支撑均匀稳定,可分散颈部的重力减少区域高压力的产生。同时,颈椎牵引体位垫的覆盖面积大,可为胸腰椎提供支撑的同时,自身重力的作用下可有效减少体位垫的移位,整块固定式设计减少颈部支撑区域的移位,减少使用过程中的剪切力及摩擦力。由于自制颈椎牵引体位垫使用加棉、加厚、透气性好的棉布覆盖于高密度海绵表面,其在使用过程中,颈部接触时减少汗液残留时间,保持背部干燥。同时在护理过程中,可简单化护理操作,较传统填充无需再行压力性损伤护理后多次调整支撑高度和位置,减少牵引效果不好的可能性。研究结果验证了自制颈椎牵引体位垫在减少压力性损伤方面的有效性,与设计初衷是契合的。
-
本研究结果中,2组研究对象在对不同颈部支撑物的评价中,观察组的舒适度评分显著高于对照组。舒适度与病人的疼痛程度相关以及接受护理过程中的方便程度相关[13-14]。自制的颈椎牵引体位垫较传统填充明显减少疼痛程度,上文已述,颈部高密度海绵的应用可保持颈部有效合理的支撑且覆以棉布增加病人主观舒适度。同时,副体垫两侧设计有拉绳,操作轴线翻身时安全性高,方便移动病人及日常床单更换,减轻了病人在护理工作时活动的负担以及护理人员的工作强度,增加了护理工作的方便性。在行牵引治疗初期,一次即可调整好颈部支撑高度,因其贴合程度良好无需在后续操作中继续调整。
自制颈椎牵引体位垫在颅骨牵引治疗中有以下特点:(1)整体分体化。自制颈椎牵引体位垫由多部分组成,使用时组装方便,易于收纳,可满足不同程度的颈椎过伸需要。(2)主体垫整体化。躯干及颈部支撑的一体化可有效避免长期牵引过程中传统巾卷变形、失支撑的缺点。(3)降低不适,提升舒适度。在颅骨牵引治疗过程中较传统填充物有效提升病人的舒适度和主观满意度,减轻病人的痛苦。(4)减少压力性损伤发生。较传统巾卷可提供有效支撑,方便护理。同时,在使用过程中需注意:(1)确保病人身体完全贴服于体位垫;(2)日常护理需挪动病人身体时使用拉绳,保持病人的身体稳定;(3)保持体位垫在使用过程中清洁、干燥,钉眼处如有渗出应及时更换;(4)牵引期间需常检查枕后、棘突处皮肤情况,预防压力性损伤的发生。
总之,自制颈椎牵引体位垫可操作性强,病人对其满意度高,可对医护的工作更加信任[15],促进了医患关系的和谐,增加了对抗疾病的信心,为病人提供了更加优质的护理服务。颈椎牵引体位垫在我科临床应用多年以来,总体效果满意,得到了病人及医务人员的一致好评,值得临床推广应用。
自制颈椎牵引体位垫在颈椎骨折伴脱位颅骨牵引治疗中的应用
Application value of self-made cervical traction pad in the skull traction treatment of cervical fracture complicated with dislocation
-
摘要:
目的探讨自行设计的颈椎牵引体位垫在颈椎骨折脱位颅骨牵引治疗中的临床应用效果。 方法选取2016年1月至2020年2月安徽省阜阳市人民医院骨科脊柱创伤病区收治的64例外伤导致颈椎骨折脱位需行颅骨牵引治疗的病人,随机分为观察组和对照组,每组32例。其中对照组在行颅骨牵引时使用传统巾卷垫于颈部,肩背部垫棉被或浴巾等物品,使胸背部抬高。观察组采用自行设计的颈椎牵引体位垫。观察并收集牵引过程次日、第4天、末次观察时SF-McGill量表评估的牵引治疗过程中病人的疼痛程度、Ⅰ期压力性损伤发生率、舒适度,统计分析其差异性。 结果SF-McGill量表评分,观察组与对照组在牵引次日差异无统计学意义(P > 0.05),在第4天及末次观察中,观察组低于对照组(P < 0.01)。观察组压力性损伤发生率低于对照组,舒适度评分高于对照组,差异均有统计学意义(P < 0.01)。 结论自制颈椎牵引体位垫在病人牵引治疗中较传统填充可减轻病人疼痛程度,减少皮肤压力性损伤的发生,提高病人牵引过程中的舒适度。 Abstract:ObjectiveTo investigate the application effects of self-made cervical traction pad in the skull traction treatment of cervical fracture complicated with dislocation. MethodsA total of 64 patients with cervical vertebra fracture complicated with dislocation caused by exceptional injury and requiring skull traction treatment in the Department of Orthopedics Spinal Trauma in Fuyang People's Hospital of Anhui province from January 2016 to February 2020 were investigated, and randomly divided into the observation group and control group(32 cases in each group). The control group was treated with the traditional towel roll to pad the neck and quilts or bath towels to pad the shoulder and back for raising the chest and back during skull traction. The observation group was treated with the self-designed cervical traction pad. The SF-McGill scale was used to evaluate the pain degree, incidence of stage Ⅰ stress injury and comfort level of patients on the next day, fourth day and last observation during traction treatment, and the differences of which were statistically analyzed. ResultsThe difference of the SF-McGill scale score on the second day of traction was not statistically between two groups(P > 0.05), and the SF-McGill scale scores in observation group on the fourth day and last observation of traction were lower than that in control group(P < 0.01). The incidence rate of stress injury and comfort score in observation group were lower and higher than that in control group, respectively(P < 0.01). ConclusionsCompared with traditional filling, the self-made cervical traction pad can reduce the pain degree and occurrence of skin pressure injury, and improve the comfort level of patients in the process of traction. -
Key words:
- skull traction /
- bed care /
- cervical traction pad
-
表 1 2组牵引期间SF-McGill量表评分及压力性损伤发生情况
分组 n SF-McGill量表评分(x±s)/分 Ⅰ期压力性
损伤发生牵引次日 第4天 末次观察 观察组 32 32.0±2.8 25.3±2.7 21.8±1.8 3 对照组 32 32.6±2.6 27.3±1.6 24.1±2.0 12 t — 0.89 3.60* 4.83 7.05# P — > 0.05 < 0.01 < 0.01 < 0.01 *示t′值; #示χ2值  下载: 导出CSV
下载: 导出CSV
-
[1] 陈举, 张朝春. 全麻下颅骨牵引复位配合颈前路减压融合治疗下颈椎骨折脱位伴关节突交锁[J]. 第三军医大学学报, 2016, 38(1): 93. [2] 沈哲, 郭伟壮, 杨欣建. 颅骨牵引复位配合前路减压融合治疗下颈椎骨折脱位伴关节突绞锁[J]. 实用骨科杂志, 2019, 25(1): 59. [3] 顾丽莉, 胡毓敏. 上颈椎不稳行后路手术患者的围手术期护理[J]. 当代护士(下旬刊), 2018, 25(12): 54. [4] 王龙强, 黄相鹏, 付松, 等. 颅骨牵引联合手法复位并手术治疗下颈椎骨折脱位合并关节突交锁的疗效观察[J]. 中国骨与关节损伤杂志, 2019, 34(5): 488. [5] 夏玉斌, 肖静蓉. 上颈椎损伤患者颅骨牵引护理体会[J]. 当代护士(下旬刊), 2017(3): 58. [6] HANSEN RB, FROST CØ, SONNE NM, et al. Exploring the patients' perception of background and breakthrough pain: A McGill pain questionnaire inquiry in patients with bone cancer pain[J]. J Palliat Med, 2019, 22(8): 881. doi: 10.1089/jpm.2018.0621 [7] National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Uleers: Quick Reference Guide[M]. Emily Haesler(Ed). Western Australia: Cambridge Media, 2014. [8] DAWES J. Do data characteristics change according to the number of scale points used An experiment using 5 point, 7 point and 10 point scales[J]. Intern J Market Res, 2008, 51(1): 1. [9] COX EP. The optimal number of response alternatives for a scale: a review[J]. J Marketing Res, 1980, 17(4): 407. doi: 10.1177/002224378001700401 [10] 刘雪晶, 杨小莹, 于梅. 集束化管理在脊柱外科2期压力性损伤患者中西医结合护理中的应用研究[J]. 现代中西医结合杂志, 2020, 29(12): 1347. doi: 10.3969/j.issn.1008-8849.2020.12.022 [11] SHI C, DUMVILLE JC, CULLUM N. Skin status for predicting pressure ulcer development: A systematic review and meta-analyses[J]. Int J Nurs Stud, 2018, 87: 14. [12] 徐慧萍, 刘延锦, 李英, 等. 改良式颈围领衬垫在颈椎术后患者中的应用及效果观察[J]. 护士进修杂志, 2018, 33(22): 95. [13] 孙丽, 顾海燕, 崔佰红, 等. 颈椎控制性轴向牵引自控器在颈椎骨折颅骨牵引患者中的应用[J]. 齐鲁护理杂志, 2018, 24(10): 40. [14] 张萍, 马杰, 邵艳. 综合护理干预对骨科患者疼痛的缓解效果[J]. 蚌埠医学院学报, 2015, 40(12): 1732. [15] 余晓燕. 综合护理模式在48例颈椎骨折脱位合并脊髓损伤病人的应用[J]. 蚌埠医学院学报, 2017, 42(6): 819. -

 点击查看大图
点击查看大图
图(2)表(1)
计量
- 文章访问数: 3788
- HTML全文浏览量: 2152
- PDF下载量: 4
- 被引次数: 0
