



-
肛瘘是常见的肛周感染性疾病,治疗以手术为主,术前手术方案制定的关键是准确定位内口及判断瘘管的数量及走形,以争取最大限度降低对肛管功能的损伤及复发率。Goodsall规律在很多外科书中被用来定位肛瘘内口,地方很多医院临床医生不做影像学检查,而仅仅根据Goodsall规律来判断内口进行手术,结果造成不必要的肛管括约肌的损伤,严重者会导致大便失禁等。本研究通过分析Goodsall规律预测肛瘘内口、超声探查肛瘘内口与手术探查结果的一致性,评估Goodsall规律预测肛瘘内口、超声定位内口的有效性,旨在临床应用中充分利用好超声检查,不要盲目依据Goodsall规律预测的内口来考虑手术方案,造成医源性损伤。现作报道。
-
选择2019年6月至2020年10月在我院行手术治疗的肛瘘病人52例,男43例,女9例,年龄15~67岁。排除标准:外口不明显,确诊或可疑克罗恩病、结核性、肿瘤性或外伤性肛瘘病人。本研究经医院伦理会批准。
-
日立ALoKA彩色多普勒超声诊断仪,经直肠变频双平面探头, 线阵探头频率:4~13 MHz,凸阵探头频率:3~9 MHz;经会阴高频探头频率:5~12 MHz, 经直肠360°探头频率:5~10 MHz。
-
术前与病人沟通检查目的,取得病人配合。两名高年资医生进行超声探查及图像分析。病人检查前排空大便,取左侧卧位,嘱病人用手协助充分暴露会阴肛门区域,先视诊肛瘘外口,根据Goodsall规律评估内口并登记;指检有无肛门狭窄、有无压痛点。使用一次性安全套保护探头,经会阴高频探头扫查,以肛门为圆心做360°扫查,记录肛瘘外口数目及距离肛缘的距离、记录瘘管肛周皮下段部分数目、位置及走向、初步判断内口的方位;用经直肠双平面探头扫查,避孕套保护探头,轻柔插入肛门;双平面线阵探头进行360°扫查,重点观察瘘管肛管深部段的走行、内口的方位、距离肛缘的距离,探查瘘管与肛管括约肌关系判断瘘管分型;使用凸阵探头或360°探头在瘘管走行区域进行来回提插扫查,补充观察。
-
观察Goodsall规律预测肛瘘内口位置、手术探查过程内口位置,记录经直肠双平面超声探查肛瘘的内口情况、瘘管的走行。
-
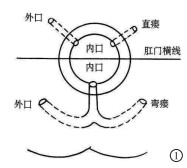
Goodsall规律: 肛门中心画一横线,外口位于横线前方的瘘管呈直管走行,外口与内口的位置相对应; 外口位于横线后方,肛瘘呈弯曲形,内口常在肛管后正中[1](见图 1)。肛瘘内口超声诊断标准:肛管黏膜或内括约肌有缺损(见图 2、3)。

图 1 Goodsall规律图

图 2 经直肠双平面超声线阵探头显示肛楼内口(白箭头示)

图 3 经直肠双平面环阵显示肛瘘内口(白箭头示)
-
采用Kappa一致性检验,Kappa一致性标准0.81~1.00代表强,0.61~0.80代表较强,0.41~0.60代表中等,0.21~0.40代表一般, < 0.20代表较差。
-
Goodsall规律预测内口与手术内口位置符合率87.1%,一致性检验Kappa值为0.657,具有较强一致性(P < 0.01)(见表 1)。
手术内口位置 Goodsall规律预测内口位置 合计 定位(+) 定位(-) 定位(+) 48 5 53 定位(-) 4 13 17 合计 52 18 70 Kappa 0.657 — P < 0.01 — 表 1 Goodsall规律预测与手术内口位置一致性检验
-
超声探查内口位置与手术内口位置符合率88.6%,一致性检验Kappa值为0.676,具有较强一致性(P < 0.01)(见表 2)。
手术内口位置 超声内口位置 合计 定位(+) 定位(-) 定位(+) 50 3 53 定位(-) 5 12 17 合计 55 15 70 Kappa 0.676 — P < 0.01 — 表 2 超声与手术探查内口位置一致性检验
-
浅表皮下瘘12条,括约肌间瘘43条,经括约肌瘘10条,括约肌上瘘2条,马蹄形瘘3条。
-
Goodsall规律对浅表皮下型、括约肌间型肛瘘内口预测与超声探查符合率90.1%,对经括约肌型、马蹄形及括约肌上型肛瘘内口预测符合率46.9%,未探查到括约肌外型肛瘘。Goodsall规律预测内口位置与超声探查内口位置一致性检验Kappa值为0.486,具有中等一致性(P < 0.05)(见表 3)。
Goodsall规律预测内口位置 超声内口位置 合计 定位(+) 定位(-) 定位(+) 47 5 52 定位(-) 8 10 18 合计 55 15 70 Kappa 0.486 — P < 0.05 — 表 3 Goodsall规律预测与超声探查内口位置一致性检验
-
本研究中所有肛瘘排除了外伤、克罗恩病、结核及肿瘤引起的肛瘘,以便观察肛瘘的真实自然形成过程。肛瘘内口开口于肛隐窝,肛隐窝为肛瓣与肛柱小袋状窝,袋口朝上,底部为肛腺开口,一般正常肛管内肛腺4~8个,多位于肛后壁,呈分支状,多位于黏膜下,也可延伸至肛旁组织,譬如括约肌间,肛腺炎引起肛周脓肿,发展为肛瘘。肛瘘的外开口位于肛周皮肤处,肉眼可见,肛瘘内口不能直接观察到,需要间接诊断,因此肛瘘内口的定位是影响手术方案及预后的关键。
Goodsall规律是1887年根据高级外科医生大卫·亨利Goodsall观察提出肛瘘的外口与内口间存在关系,根据外口推测内口位置,对发现肛瘘内口起到很大帮助,但在本研究中发现虽然根据Goodsall规律推导肛瘘内口位置与手术结果或超声探查结果一致性较高,具有一定临床价值,但在手术探查过程中,尤其是对比经直肠双平面超声中发现Goodsall规律有一定局限性。
本研究并未将手术探查结果作为金标准,因为临床手术可能会经验性地根据Goodsall规律去探查内口,结果会造成医源性假性内口,本研究结果也显示Goodsall规律与手术结果的一致性高于Goodsall规律与超声结果的一致性,超声结果对于肛瘘内口的显示反而具有一定的客观性,采用经直肠双平面超声探查中发现部分瘘管并非如Goodsall规律所提:外口位于中线前的瘘管呈直管,内口开口于对应钟点的肛管内壁处,观察结果显示其中有6例女性病人的6条肛瘘外口虽位于横线之前、中线以外的位置,内口却均开口于前中线处,另有2例病人的2条瘘管的外口位于横线之前中线以外钟点,内口有2个,一个内口位置如Goodsall所推导位置位于对应钟点,另一分支瘘管却呈弯曲瘘、内口位置却位于前中线处,因此并不是全如Goodsall规律所推测的结果,关于Goodsall规律准确性研究报道并不多,本研究与AYARAJAH等[2]一项研究相似,该研究指出Goodsall规律对外开口在横线前的肛瘘内口预测准确率低于位于后面开口瘘。无论是前中线还是后中线肛隐窝,都是肛瘘主要的起源地,与继发外口的位置无关,很多横线前肛瘘,无论外口位于前中线处,或是前中线以外,内口也开口于前中线处。此点挑战了Goodsall规律的预测性[3-6]。当时Goodsall规律的提出缺乏支持数据,1906年63岁Goodsall死于心肌梗死,距他教科书出版仅仅6年,因此留下很多未解之谜[1]。
本研究中经直肠双平面超声与手术结果具有较强的一致性,经直肠双平面探头位于侧边,垂直肠壁,紧贴肠壁排除气体干扰,且其频率范围属于高频超声(线阵探头频率为4~13 MHz,环阵探头频率为3~9 MHz),具有较高的分辨率,可清晰显示肛管壁从内向外的5层结构:黏膜层、肛管内括约肌、联合纵肌、外括约肌及肛周脂肪间隙,可判断肛瘘的Parks分型[7-10],同时内口的显示率大幅提高,可准确测量内口与肛缘间的距离,为手术提供精准预判,这些均是Goodsall规律评估不了的。本研究中瘘管类型主要为浅表皮下型和括约肌间型,Goodsall推测此类肛瘘内口位置与手术、超声符合率较高,对于括约肌上型和马蹄形瘘预测符合率低,低于超声评估肛瘘内口的准确性,此次观察结果中特殊类型肛瘘病例较少,未发现到括约肌外形肛瘘,也是本研究的不足之处。金玉明等[11]报道二维超声对肛瘘内口诊断符合率结果为Kappa系数0.48。程素萍等[12]报道经直肠双平面腔内超声诊断内口的灵敏度98.3%,特异度98.0%。
因此,超声医生可在充分了解Goodsall规律优势的情况下,一定程度上可指引超声探查肛瘘内口,特别在寻找纤细或者超声上灰度对比度不明显甚至有着多个细支瘘的复杂性肛瘘的内口上可以起到一定帮助;另外充分了解Goodsall规律的局限性,临床手术不盲从该规律,必须利用好经直肠双平面腔内超声探查肛瘘内口的优势来指导临床手术方案,减少再次手术机会,降低肛门功能损伤的发生率。
Goodsall规律预测与经直肠双平面腔内超声定位肛瘘内口的价值比较
Comparison of the value of the Goodsall rule and biplane transrectal ultrasonography in positioning the internal opening of anal fistula
-
摘要:
目的评估Goodsall规律预测肛瘘内口、经直肠双平面超声定位肛瘘内口的价值。 方法回顾性分析行手术治疗的肛瘘病人52例(70条肛瘘)临床资料, 每例病人术前均根据Goodsall规律预测肛瘘内口, 同时行经直肠双平面超声探查内口, 并与手术探查结果进行一致性检验比较。 结果Goodsall规律预测与手术符合率87.1%, 一致性检验Kappa值为0.657, 具有较强一致性(P < 0.01)。超声探查内口和手术诊断符合率88.6%, 一致性检验Kappa值为0.676, 具有较强一致性(P < 0.01)。70条肛瘘超声探查结果: 浅表皮下瘘12条, 括约肌间瘘43条, 经括约肌瘘10条, 括约肌上瘘2条, 马蹄形瘘3条。Goodsall规律对浅表皮下型、括约肌间型肛瘘内口预测与超声探查符合率较高(90.1%), 对经括约肌型、马蹄形及括约肌上型肛瘘内口预测符合率不高(46.9%), 一致性检验Kappa值为0.486, 具有中等一致性(P < 0.05)。 结论Goodsall规律预测肛瘘内口与手术或经直肠双平面超声具有高度一致性, 具有一定临床价值, 尤其对浅表皮下型瘘、括约肌间型瘘预测与超声符合率较高, 但在预测外口位于横线前的瘘管及马蹄形型、经括约肌型、括约肌上型瘘内口位置有一定局限性; 超声探查及临床治疗中可将Goodsall规律与经直肠双平面超声有效结合, 提高诊断及治疗效果。 -
关键词:
- 肛瘘 /
- 经直肠双平面超声 /
- Goodsall规律
Abstract:ObjectiveTo evaluate the value of the Goodsall rule in predicting internal opening of anal fistula and the value in locating the internal opening of anal fistula using biplane transrectal ultrasonog raphy. MethodsThe clinical data of 52 patients(70 anal fistulas) who underwent surgical treatment were retrospectively analyzed.The internal opening of anal fistula of each patient was predicted according to the Goodsall rule before surgery, and the internal fistula was simultaneously explored by biplane transrectal ultrasonography.Both results were compared with surgical exploration results via a consistency test. ResultsThe consistency rate of the Goodsall rule and operation diagnosis was 87.1%, and the Kappa value in the consistency test was 0.657, showing strong consistency(P < 0.01).The consistency rate of ultrasonic exploration and surgical diagnosis was 88.6%, and the Kappa value in the consistency test was 0.676, showing strong consistency(P < 0.01).Results of ultrasonic exploration of 70 anal fistulas were listed as follows: 12 superficial subcutaneous fistulas, 43 intersphincteric fistulas, 10 transsphincteric fistulas, 2 superior sphincteric fistulas and 3 horseshoe fistulas.The Goodsall rule had a high coincidence with ultrasonic exploration for superficial subcutaneous, intersphincteric anal fistulas and ultrasonic probe(90.1%).However, the prediction rate of the Goodsall rule for the internal opening of transsphincter type, horseshoe type, and suprasphincter type was not high(46.9%), and the Kappa value of consistency test was 0.486, showing moderate consistency(P < 0.05). ConclusionsThe value of the Goodsall rule in predicting the internal opening is highly consistent with surgery or biplane transrectal ultrasonography, showing a certain clinical value, especially for superficial subcutaneous fistula and intersphincteric anal fistulas, whereas there are some limitations in predicting the location of fistulas in front of the transverse line and the internal opening of horseshoe, transsphincter, and suprachincter fistulas.In ultrasound examination and clinical treatment, the Goodsall rule can be effectively combined with biplane transrectal ultrasonography to improve the diagnosis and treatment effect. -
Key words:
- anal fistula /
- biplane transrectal ultrasonography /
- Goodsall rule
-
表 1 Goodsall规律预测与手术内口位置一致性检验
手术内口位置 Goodsall规律预测内口位置 合计 定位(+) 定位(-) 定位(+) 48 5 53 定位(-) 4 13 17 合计 52 18 70 Kappa 0.657 — P < 0.01 —  下载: 导出CSV
下载: 导出CSV
表 2 超声与手术探查内口位置一致性检验
手术内口位置 超声内口位置 合计 定位(+) 定位(-) 定位(+) 50 3 53 定位(-) 5 12 17 合计 55 15 70 Kappa 0.676 — P < 0.01 —
下载: 导出CSV
表 3 Goodsall规律预测与超声探查内口位置一致性检验
Goodsall规律预测内口位置 超声内口位置 合计 定位(+) 定位(-) 定位(+) 47 5 52 定位(-) 8 10 18 合计 55 15 70 Kappa 0.486 — P < 0.05 —
下载: 导出CSV
-
[1] MALLICK KK. Relevance of Goodsall's rule in fistula-in-ano[J]. IOSR J Pharmacy (IOSRPHR), 2013, 3(7): 20. doi: 10.9790/3013-0371020-22 [2] AYARAJAH U, SAMARASEKERA DN. Predictive accuracy of Goodsall's rule for fistula-in-ano[J]. Ceylon Med J, 2017, 62(2): 97. doi: 10.4038/cmj.v62i2.8474 [3] CIROCCO WC, REILLY JC. It is time to retire Goodsall's rule: the midline rule is a more accurate predictor of the true and natural course of anal fistulas[J]. Tech Coloproctol, 2020, 24(4): 317. doi: 10.1007/s10151-020-02167-z [4] MURALIDHAR V, SANTHASEELAN RG, KRISHNAMURTHY A. Long anterior anal fistula with an external opening in the medial raphe of the scrotum is likely to open radially inside the anal canal: an addition to the Goodsall's rule[J]. BMJ Case Rep, 2018, 2018: 1. [5] CIROCCO WC. Goodsall's flaw[J]. Tech Coloproctol, 2020, 24(7): 777. doi: 10.1007/s10151-020-02236-3 [6] GUNAWARDHANA PA, DEEN KI. Comparison of hydrogen peroxide instillation with Goodsall's rule for fistula in ano[J]. Anz J Surg, 2015, 71(8): 472. [7] 吴长君. 超声诊断与解剖图谱[M]. 北京: 人民卫生出版社, 2011: 85. [8] 刘得超, 李文儒, 王馨华, 等. 肛瘘磁共振成像分型[J]. 中华胃肠外科杂志, 2018, 21(12): 1391. [9] 吴长君, 吴国柱, 刘银龙, 等. 经直肠双平面腔内超声对肛瘘及其分型的诊断价值[J]. 中国超声医学杂志, 2011, 27(10): 932. [10] PARKS AG, GORDON PH, HARDCASTLE JD. A classification of fistula in ano[J]. British J Surg, 1976, 63(1): 1. [11] 金玉明, 黄婷, 洪桂荣. 经直肠腔内超声诊断肛瘘临床价值[J]. 中国超声医学杂志, 2019, 35(10): 940. [12] 程素萍, 刘娟, 吴中权. 经直肠双平面腔内超声诊断肛瘘的价值[J]. 中国超声医学杂志, 2015, 31(8): 731. -

 点击查看大图
点击查看大图
图(3)表(3)
计量
- 文章访问数: 3653
- HTML全文浏览量: 1515
- PDF下载量: 7
- 被引次数: 0
