

-
鼓膜穿孔的原因很多,慢性化脓性中耳炎是其常见病因之一[1],其次多为外伤性或医源性。传统的手术治疗方式多为显微镜下耳后入路行单纯鼓膜修补或乳突鼓室手术,修补材料为颞肌筋膜、脂肪组织、乳突骨膜等[2-3],多为就近取材。近年来随着耳内镜的发展,依据其广角和多角度的优点,在内镜下经外耳道的自然通道入路,可以清晰地显示鼓室内的各个解剖部位及病变情况,并能很好地清除病变。在耳内镜下的鼓室成形中所用的修补材料就近多为耳屏软骨(包含或不包含软骨膜),然而鼓膜穿孔的大小和类型是多样的,适合的耳屏软骨-软骨膜制作对于穿孔的愈合及术后听力的影响尤为重要。为此,我们选择在耳内镜下完成鼓室探查+不同类型的鼓室成形术的病人,回顾性分析不同类型的耳屏软骨-软骨膜修补鼓膜穿孔情况。现作报道。
-
收集2018-2021年我科住院并接受耳内镜下中耳手术共60例(60耳)病人的临床资料,其中男29例,女31例,年龄18~69岁。纳入标准:所有病人术前颞骨CT显示病变局限于鼓室内,乳突内无不可逆性病变。本研究经医院伦理委员会同意。临床诊断为慢性化脓性中耳炎58例,其中2例合并鼓室硬化;外伤性鼓膜穿孔2例。依据病情行鼓室成形术Ⅰ型50例,鼓室成形术Ⅱ型10例。所有病例均由同一治疗组医生完成, 将60例随机分为对照组和观察组,各30例。2组性别、年龄、鼓室成形术分型均具有可比性。
-
内镜摄像及监视系统(德国Storz公司);耳内镜(φ3mm,0°和45°);耳科显微手术器械,所有病人均在全麻下进行。
-
对照组使用全厚岛状耳屏软骨-软骨膜修补鼓膜穿孔;观察组使用半厚岛状耳屏软骨-软骨膜复合体修补鼓膜穿孔。具体操作如下:所有病人均在全身麻醉下进行,含0.1%肾上腺素0.9%氯化钠溶液于外耳道骨膜下局部浸润后,经耳道内切口入路,环切刀于外耳道后壁距离鼓环约15 mm处切开,上至12点方向,下至6点方向处,分离外耳道皮肤形成皮瓣,掀起鼓环进入鼓室腔。(1)鼓室无病变,采用0°耳内镜下完成,探查鼓室腔内黏膜正常,听骨链完整,分离并暴露鼓索神经予以保护,去除陈旧性的穿孔边缘及锤骨柄的上皮组织,修建新鲜血床。(2)鼓室有病变则采用0°和45°耳内镜下完成。依据鼓室病变情况行鼓室探查+鼓室成形术(Ⅰ型或Ⅱ型),进入鼓室腔,分离并暴露鼓索神经予以保护,刮匙或电钻磨除上鼓室外侧壁部分骨质,充分暴露上鼓室,去除其内病变(肉芽或胆脂瘤上皮等),并探查听骨链完整性及活动度良好,行鼓室成形术Ⅰ型;探查锤砧关节、砧镫关节固定或听骨破坏者,离断其关节后探查锤骨及镫骨底板活动度及镫骨活动均良好,两窗功能正常,去除固定及破坏听骨,探查并清除上鼓室、后鼓室病变,行鼓室成形术Ⅱ型。于同侧耳屏处取耳屏软骨膜,对照组制作成全厚岛状耳屏软骨膜以内置法修补鼓膜,观察组制作成半厚岛状耳屏软骨-软骨膜复合体(见图 1),其中半厚岛状耳屏软骨膜以内置法修补穿孔鼓膜处,分离出的单纯软骨膜则以外置法修补缺损处不留缝隙。所有病人均行明胶海绵及碘仿纱条填塞外耳道;乙醇棉球填塞外耳道口压迫耳屏内侧切口。小敷料覆盖外耳道口。

图 1 半厚双岛耳屏软骨膜
-
术后2周抽出外耳道填塞物及耳屏处缝线。术后1、3、6个月复查,电子耳镜下观察鼓膜生长情况,测试纯音测听观察听力恢复情况。
-
采用t检验和Fisher′s确切概率法。
-
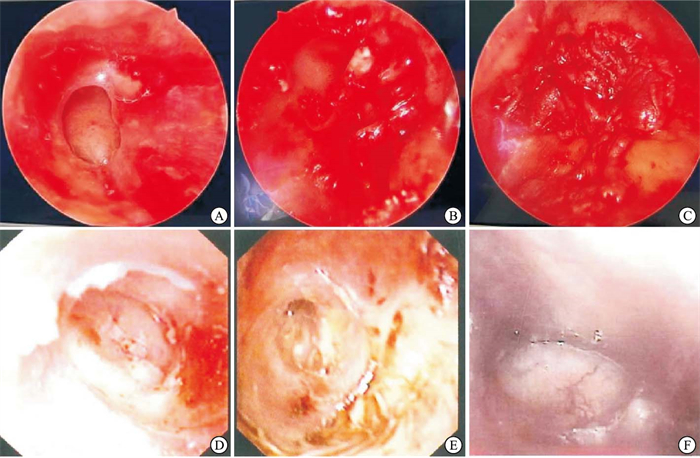
所有病人随访6~12个月,对照组鼓膜愈合24例(80.0%), 大穿孔变小穿孔6例(20.0%)。观察组鼓膜愈合30例(100%),5例出现感染情况,外耳道见脓性分泌物,经抗感染及对症处理后,1个月后逐渐干耳;1例病人出现耳屏处青紫,可能是外耳道口压迫不紧所致,1周后青紫慢慢消退无感染征象。2组鼓膜愈合率差异有统计学意义(Fisher′s确切概率法,P < 0.05)。所有病人未出现感音神经性聋、周围性面瘫等严重并发症。术中及术后鼓膜图情况见图 2。

图 2 手术前后病人鼓膜情况
-
术前及术后通过纯音测听结果比较听力情况。2组术前气导听阈、气骨导差值差异均无统计学意义(P>0.05),术后6个月观察组气导听阈、气骨导差值均明显优于对照组(P < 0.01), 且组内比较结果显示,术后6个月2组气导听阈、气骨导差值均明显优于术前(P < 0.01)(见表 1)。
分组 n 气导听阈/dB 气骨导差/dB 术前 对照组 30 45.6±8.6 21.4±4.8 观察组 30 43.2±5.2 20.1±3.6 t — 1.31 1.19 P — >0.05 >0.05 术后6个月 对照组 30 34.9±7.8** 12.1±1.9** 观察组 30 28.9±3.1** 9.3±2.1** t — 3.92 5.42 P — < 0.01 < 0.01 组内配对t检验:**P < 0.01 表 1 2组病人手术前后纯音测听结果比较(x±s)
-
传统的中耳手术多在显微镜下进行,多取耳后切口,通过研磨乳突进入鼓窦及鼓室腔,进行清理病变及依据病变情况做不同类型的鼓室成形,疗效是确切的。但是其手术条件要求较高,需要性能较好的显微镜、不同类型的高速电钻及不同的变换病人的头位才能更好地完成手术。另外其光线是固定直线光轴,后下鼓室几乎是盲区,这也是中耳手术易复发的主要原因。而耳内镜具有广角和多角度的优势,通过外耳道的自然通道入路其符合目前微创手术理念,通过不同角度的耳内镜进入鼓室腔后几乎可以观察鼓室内所有解剖结构,如咽鼓管鼓口、听骨链、鼓索神经、面神经等,尤其在显微镜下不好暴露的面隐窝、鼓室窦、后鼓室、盾板内侧等解剖部位[4],在耳内镜下结合内镜摄像及监视系统均可以很好地显露。本组术中60耳均可在耳内镜下非常好地暴露病变,并彻底清除病变。另外术中不受病人体位变化影响,术者手术操作较为灵活,可以避免开放乳突的巨大磨骨量,缩短手术时间并减少术中出血量。
鼓室成形术是中耳炎手术分型一种方式,其目的就是改善病人听力,临床分为3型[5],依据病变残余情况做不同类型的鼓室成形,本组病人60耳中以单纯型慢性化脓性中耳炎为主58耳(96.7%),鼓膜外伤性穿孔2耳(3.3%);病人术前均行颞骨CT排除鼓窦及乳突病变。病变局限在鼓室腔内是耳内镜手术的最佳适应证。目前耳内镜下较多的是Ⅰ、Ⅱ型鼓室成形,鼓室成形Ⅰ型主要针对鼓室腔黏膜正常,听骨链完整的单侧鼓膜穿孔,其引起原因多有鼓膜外伤、单纯性中耳炎等。鼓室成形Ⅱ型主要针对镫骨上结构部分破坏的病变,其多有炎性肉芽或胆脂瘤引起,因为听骨链部分破坏吸收,多需要重建听骨链,如自体残余听骨或人工听骨等。本组病人中鼓室成形Ⅰ型有50例(83.3%),鼓室成形Ⅱ型有10例(16.7%)。
鼓室成形的鼓膜修补材料有很多,如颞肌筋膜、耳屏软骨膜、人工脑膜、人工羊膜等[2]。应用最多的为颞肌筋膜和耳屏软骨膜,针对耳内镜下的鼓膜修补材料,我们所有修补材料的选择为自体耳屏软骨膜,其成功率较颞肌筋膜要高[6-7]。因耳屏软骨-软骨膜具有很多的特点如:(1)具有一定的弹性和硬度,这种特点使得鼓室腔容积固定,不易粘连,可防止术后鼓室粘连、鼓膜萎缩及内陷袋形成。(2)就近取材,手术切口仅在耳屏及外耳道内段,手术创伤小,耳屏内切口仅缝合1~2针,因切口隐蔽、术后瘢痕小,愈合后外观无伤口,符合美容微创要求。(3)耳屏软骨-软骨膜成活率高,其可从鼓室渗出液中汲取营养,从而抵抗感染和血供不足的情况。因此无论干耳或湿耳情况,鼓室病变彻底清除后,其都可以应用,大大提高了手术适应证[8]。
目前国内外有多种类型自体耳屏软骨膜的应用[9-10],如全厚软骨-软骨膜、岛状软骨-单层软骨膜、岛状软骨-双层软骨膜等,每种类型软骨膜各有优缺点。为此我们选择2组不同类型的耳屏软骨-软骨膜做比较,发现全厚软骨-软骨膜虽具有良好的韧性及形态,但尺寸大小受限、厚度不一,容易出现修补缺损,术后因贴补有缝隙或偏移再穿孔的概率发生较高(20%)。同时也出现听力提高较慢等情况[11-12]。而通过我们制作的半厚岛状耳屏软骨-软骨膜复合体既解决了缺损鼓膜大小尺寸的问题,又能很短时间提高病人的听力,同时成活率也较高。尤其在制取耳屏软骨-软骨膜时,我们取的是双层软骨膜和软骨的复合体,通过修剪成半厚岛状耳屏软骨-软骨膜复合体,半厚岛状耳屏软骨-软骨膜以内置法主要修补穿孔的大部分区域,边缘区域则以修剪出的单纯软骨膜以内植法、外植法进行修补,通过随访鼓膜愈合率达到100%。半厚岛状耳屏软骨-软骨膜因其厚度较全厚软骨膜的厚度减半,我们通过术后6个月左右的纯音测听结果进行比较分析,结果显示无论气导听阈还是气骨导差,半厚岛状耳屏软骨-软骨膜均优于全厚软骨膜,术后听力改善明显。
综上,耳内镜下耳屏软骨膜修补鼓膜并行不同类型鼓室成形,手术安全、创伤小,可获得较高的手术成功率。当然其局限性也是明显的,如单手操作,手术操作空间较小,镜面易污染等特点,且外耳道狭窄及出血明显后无法完成手术,手术适应证局限于鼓室内病变等。但其可视性强,有多规格视角物镜,可以对深腔侧方视野进行处理,手术硬件要求不高,仅需耳内镜和可视系统及耳科显微器械就可开展手术。随着内镜技术的广泛开展,很多基层医院就可以开展此类技术,因此利于临床推广。
耳内镜下不同类型耳屏软骨-软骨膜修补鼓膜穿孔临床疗效分析
Clinical effect analysis of repairing tympanic membrane perforation with different types of tragus cartilage-perichondrium under otoendoscope
-
摘要:
目的探讨耳内镜下不同类型的耳屏软骨-软骨膜修补鼓膜穿孔的临床疗效。 方法选取60例(60耳)实施耳内镜手术的病人,随机分为对照组和观察组各30例,其中对照组采用全厚岛状耳屏软骨-软骨膜修补鼓膜穿孔;观察组采用半厚岛状耳屏软骨-软骨膜复合体修补鼓膜穿孔。所有病人随访6~12个月,对比分析2组鼓膜穿孔的鼓膜愈合情况及听力改善情况。 结果观察组鼓膜愈合率100.0%(30/30),高于对照组80.0%(24/30)(P < 0.05)。2组术前气导听阈、气骨导差值差异均无统计学意义(P>0.05),术后观察组气导听阈、气骨导差值均明显优于对照组(P < 0.01), 且组内比较结果显示,术后2组气导听阈、气骨导差值均明显优于术前(P < 0.01)。 结论耳内镜下耳屏软骨-软骨膜修补穿孔的鼓膜是可行的,尤其半厚岛状耳屏软骨-软骨膜复合体成活率高,可修补不同大小的鼓膜穿孔,且益于提高听力,术后听力改善效果良好。 Abstract:ObjectiveTo investigate the clinical efficacy of repairing tympanic membrane perforation with different types of tragus cartilage-perichondrium under otoendoscope. MethodsSixty patients (60 ears) who underwent endoscopic surgery were randomly divided into the control group (n=30) and the observation group (n=30).In the observation group, the perforation of tympanic membrane was repaired by semi-thick island of tragus cartilage-perichondrium complex.All patients were followed up for 6-12 months.The healing of tympanic membrane and hearing improvement were compared between the two groups. ResultsThe healing rate of tympanic membrane in the observation group was 100.0% (30/30), which was higher than 80.0%(24/30) in the control group (P < 0.05).There was no significant difference in the air-conductance threshold and air-bone conductance difference between the two groups before operation (P>0.05).The air-conductance threshold and air-bone conductance difference of the observation group were significantly better than those of the control group (P < 0.01), and the intra-group comparison showed that the air-conductance threshold and air-bone conductance difference of the two groups after operation were significantly better than those before operation (P < 0.01). ConclusionsIt is feasible to repair the perforated tympanic membrane under otoendoscope, especially the semi-thick island of auricular cartilage-perichondrium complex, which has a high survival rate, can repair the perforation of tympanic membrane of different sizes, and is beneficial to improve hearing, and the postoperative hearing improvement effect is good. -
Key words:
- tympanic membrane perforation /
- otoendoscope /
- tragus and perichondrium /
- tympanoplasty
-
表 1 2组病人手术前后纯音测听结果比较(x±s)
分组 n 气导听阈/dB 气骨导差/dB 术前 对照组 30 45.6±8.6 21.4±4.8 观察组 30 43.2±5.2 20.1±3.6 t — 1.31 1.19 P — >0.05 >0.05 术后6个月 对照组 30 34.9±7.8** 12.1±1.9** 观察组 30 28.9±3.1** 9.3±2.1** t — 3.92 5.42 P — < 0.01 < 0.01 组内配对t检验:**P < 0.01  下载: 导出CSV
下载: 导出CSV
-
[1] 张金平, 谢记发, 罗许勇. 耳内镜下耳屏软骨-软骨膜鼓膜成形术的手术技巧及疗效分析[J]. 中国中西医结合耳鼻咽喉科杂志, 2020, 28(6): 401. [2] 姜妍, 李江平, 王鹏举. 耳内镜下鼓室成形术鼓膜穿孔修复材料的比较[J]. 听力学及言语疾病杂志, 2019, 27(6): 623. [3] MOHANTY S, MANIMARAN V, UMAMAHESWARAN P, et al. Endoscopic cartilage versus temporalis fascia grafting for anterior quadrant tympanic perforations—a prospective study in a tertiary care hospital[J]. Auris Nasus Larynx, 2018, 45(5): 936. doi: 10.1016/j.anl.2018.01.002 [4] 张静, 李希平. 耳内镜下鼓室成形术临床疗效分析[J]. 解放军医学院学报2019, 40(5): 441. [5] 中华医学会耳鼻咽喉头颈外科学分会耳科学组, 中华耳鼻咽喉头颈外科杂志编辑委员会耳科组. 中耳炎临床分类和手术分型指南(2012)[J]. 中华耳鼻咽喉头颈外科杂志, 2013, 48(2): 5. [6] 潘晓丹, 赵守琴, 赵燕玲, 等. 耳内镜下内衬法与夹层法鼓膜修补术的疗效观察[J]. 中国耳鼻咽喉颅底外科杂志, 2022, 28(1): 69. [7] 熊辉强, 魏小林. 耳内镜下耳屏软骨-软骨膜在湿耳鼓室成形术中的疗效观察[J]. 江西医药, 2021, 56(1): 87. [8] JALALI MM, MOTASADDI M, KOUHI A, et al. Comparison of cartilage with temporalis fascia tympanoplasty: a meta-analysis of comparative studies[J]. Laryngo Scope, 2017, 127(9): 2139. [9] 杨启梅, 张文, 韩想利, 等. 耳内镜下耳屏软骨-软骨膜治疗鼓膜穿孔的临床研究[J]. 中华耳科学杂志, 2016, 14(6): 778. [10] NEUMANN A, HENNIG A, SCHULTZ-COULON HJ. Morphological and functional results of palisade cartilage tympanoplasty[J]. HNO, 2002, 50 (10): 935. [11] 谭志强, 刘映辰, 刘斌, 等. 耳内镜下软骨岛技术结合栅栏软骨技术修补鼓膜次全穿孔的临床研究[J]. 临床耳鼻咽喉头颈外科杂志, 2021, 35(11): 1009. [12] 张文伟, 刘稳, 刘后广, 等不同材料修补不同面积中央性鼓膜穿孔的有限元模型分析[J]. 听力学及言语疾病杂志, 2022, 30(1) : 58. -

 点击查看大图
点击查看大图

图(2)表(1)
计量
- 文章访问数: 2158
- HTML全文浏览量: 1309
- PDF下载量: 20
- 被引次数: 0
