

-
黏膜下子宫肌瘤是子宫肌瘤中的常见类型,其肌瘤生长位置位于子宫内膜下,凸向宫腔并压迫子宫内膜,引起月经改变等相关症状。黏膜下肌瘤主要分为3种类型:0型肌瘤,完全生长在子宫腔内;Ⅰ型肌瘤,部分凸向宫腔,位于肌层部分不超过50%;Ⅱ型肌瘤,少部分凸向宫腔,位于肌层内超过50%[1]。目前黏膜下肌瘤的治疗仍以宫腔镜手术为主,具有创伤小,出血少,手术时间短,不破坏子宫整体肌层结构等多重优势[2]。但宫腔镜术后有时发生相关严重并发症,主要是手术医生未能规范化进行学习和掌握该术式,因此,本研究收集同一组医生完成的宫腔镜下子宫黏膜下肌瘤切除术的相关数据,利用移动平均法拟合学习曲线[3-4],为基层医院妇产科医生学习该项技术提供参考,以期更好地为黏膜下子宫肌瘤病人服务。
-
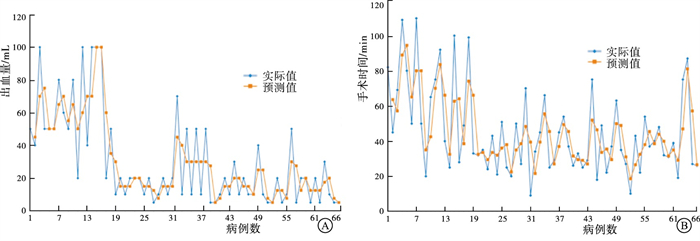
收集2018年8月至2022年3月我科同一组手术团队完成的宫腔镜下黏膜下子宫肌瘤切除术病人66例相关临床数据,按照手术时间前后进行排序编号。根据手术时间、术中出血量指标,参考既往学习曲线研究[5-6],采用移动平均法拟合学习曲线,在完成约20例手术后,手术时间逐渐稳定在40 min左右,手术出血量稳定在20 mL左右,因此,以拟合曲线中第20例手术病人为截点,将66例病人分为前1~20例(A组)和第21~66例(B组)(见图 1)。2组的病人年龄、肌瘤最大径和术前D-二聚体、血红蛋白水平及肌瘤分型差异均无统计学意义(P>0.05)(见表 1),具有可比性。

图 1 移动平均法拟合的66例宫腔镜下黏膜下肌瘤切除术学习曲线
分组 n 年龄/岁 肌瘤最大径/cm D-二聚体/(mg/L) 血红蛋白/(g/mL) 肌瘤分型 0型 Ⅰ型 Ⅱ型 A组 20 49.62±7.23 3.02±1.33 0.41±0.21 118.93±18.62 1(5) 11(55) 8(40) B组 46 49.34±9.35 3.02±1.01 0.38±0.16 118.13±18.59 3(6.5) 27(58.7) 16(34.8) t — 0.12 0.00 0.64 1.16 0.19△ P — >0.05 >0.05 >0.05 >0.05 >0.05 △示校正χ2值 表 1 2组病人一般资料比较(x±s)
-
术前完善超声检查,确定子宫肌瘤类型,并完善其他检查,排除手术禁忌,进行医患沟通并签署知情同意。术前2 h阴道放置米索前列醇软化宫颈。进行硬膜外麻醉或静脉麻醉,常规消毒阴道并扩张宫颈,经宫颈置入宫腔电切镜进行操作,尽可能促使肌瘤凸向宫腔,并结合钳夹,减少内膜损伤和过度膨宫液体灌入。
-
比较2组病人手术时间、术中出血量和术后血红蛋白、D-二聚体水平及住院时间、并发症发生情况(血尿、发热>38.5 ℃、下肢静脉血栓、低钾血症等)、月经恢复时间、月经量、术后妊娠结局。
-
采用t检验、χ2检验和Fisher′s确切概率法。
-
A组病人手术时间、术中出血量、住院时间均大于B组(P < 0.05~P < 0.01),2组术后并发症发生情况差异无统计学意义(P>0.05)(见表 2)。
分组 n 手术时间/min 术中出血量/mL 住院时间/d 术后并发症 血尿 发热 下肢深静脉血栓 低钾血症 A组 20 61.22±28.54 56.91±30.19 7.18±2.36 1 3 0 0 B组 46 37.14±17.18 16.90±14.49 6.02±1.40 0 2 1 1 t — 4.24 7.30 2.49 1.67△ P — < 0.01 < 0.01 < 0.05 >0.05 △示校正χ2值 表 2 2组病人手术相关指标比较(x±s)
-
2组病人术后月经恢复时间、月经量和术后1个月血红蛋白水平及术后随访妊娠结局差异均无统计学意义(P>0.05)(见表 3)。
分组 n 月经恢复时间/d 月经量/mL 血红蛋白浓度/(g/L) 术后随访妊娠 A组 20 28.46±12.11 46.46±29.87 129.33±18.86 1(5.00) B组 46 25.33±8.59 51.13±32.36 131.25±21.31 2(4.35) t — 1.20 0.55 0.35 — P — >0.05 >0.05 >0.05 >0.05△ △示Fisher′s确切概率法 表 3 2组病人术后恢复及随访指标比较(x±s)
-
随着宫腔镜手术技术不断发展,宫腔镜下子宫肌瘤切除术已成为有症状子宫黏膜下肌瘤病人的首选治疗方法[7]。其手术时间短,痛苦小,住院时间短,恢复快,使得宫腔镜手术成为现代妇产科医生必须掌握的手术技能之一。但任何手术技术的掌握,都需要一定手术病例和学习时间的积累。赵卫东等[5]分析腹腔镜下复杂子宫肌瘤切除术学习曲线,认为经过40例手术后,手术医生的手术时间趋于平稳。LEE等[8]分析单孔腹腔镜下子宫肌瘤切除术学习曲线,认为在45例手术后,手术医生的手术经验和能力得到了充分加强,可完全掌握该项技术。本研究中,通过移动平均法拟合手术时间和手术出血量分析显示,在约20例宫腔镜下子宫肌瘤切除术后,手术医师可基本掌握该项技术,手术时间和术中出血量均趋于平稳。这可能与本中心为基层县市级医院、适应证把控严格、整体手术难度偏低等有关,但这也为基层医院开展该项工作提供较好参考,应在宫腔镜手术开展初期,严格把控手术指征,保证病人手术安全。
学习曲线的相关影响因素较多,其中最主要的指标是手术时间[5-6, 9-10]和术中出血量[5]。基于此,本研究分别根据手术时间和术中出血量,采用移动平均法拟合学习曲线,将病人分为第1~20例(A组)和第21~66例(B组),结果显示,2组手术时间、术中出血量和住院时间差异均有统计学意义,而术后并发症差异无统计学意义。但学习曲线仍然还受到术者学习能力、病人本身因素等多方面因素影响。本研究将宫腔镜下子宫肌瘤切除术学习曲线初步定于20例,并经前后两个阶段比较分析进行验证,结果显示基本符合学习曲线的判定,但由于宫腔镜手术方面学习曲线研究较少,仍需更多研究来进一步验证。
综上,宫腔镜下子宫肌瘤切除术需经过约20例手术操作学习后,可初步掌握该项技术,术者在学习和掌握该项技术时亦需充分评估病人的病情和手术适应证,做好术前准备和应激预案,充分做好与手术护士和麻醉医师的沟通工作,才能更好地完成手术。
宫腔镜黏膜下子宫肌瘤切除术的学习曲线分析
Learning curve analysis of hysteroscopic submucosal myomectomy
-
摘要:
目的利用预测分析模型拟合宫腔镜黏膜下子宫肌瘤切除术的学习曲线,为基层医院开展宫腔镜下黏膜下子宫肌瘤切除术的学习过程提供参考。 方法收集66例行宫腔镜下黏膜下子宫肌瘤切除术病人,按照手术时间前后顺序进行编号,通过移动平均法分别根据术中出血量、手术时间拟合学习曲线,将病人分为第一阶段组(第1~20例,A组)和第二阶段组(第21~66例,B组),比较2组病人手术相关指标。 结果A组病人手术时间、术中出血量、住院时间均大于B组(P < 0.05~P < 0.01),2组术后并发症发生情况差异无统计学意义(P>0.05)。2组病人术后月经恢复时间、月经量和术后1个月血红蛋白水平及术后随访妊娠结局差异均无统计学意义(P>0.05)。 结论经过前20例宫腔镜黏膜下子宫肌瘤切除术学习阶段后,手术操作相对稳定,宫腔镜黏膜下子宫肌瘤切除术初学者应在前20例手术中严格把握适应证,熟练手术操作,学习处理突发情况,以更好地掌握手术技术。 Abstract:ObjectiveTo use the predictive analysis model to match the learning curve of hysteroscopic submucosal myomectomy, and provide a reference for learning the process of hysteroscopic submucosal myomectomy in primary hospitals. MethodsClinical data of 66 cases who underwent hysteroscopic submucosal myomectomy was selected.The patients were numbered according to the sequence of the operation time, and the learning curve was plotted according to the intraoperative blood loss and the operation time by the moving average method.The patients were divided into the first stage group (1-20 cases, group A) and the second stage group (21-66 cases, group B), and the operation related indicators of the patients in the two groups were compared. ResultsThe operation time, intraoperative blood loss and hospitalization time of patients in group A were greater than those in group B (P < 0.05 to P < 0.01), and there was no significant difference in postoperative complications between the two groups (P>0.05).There was no significant difference in the recovery time of menstruation, the amount of menstruation, the hemoglobin level in the first month after operation and the pregnancy outcome after follow-up between the two groups(P>0.05). ConclusionsAfter the learning stage of 20 surgeries, the surgical technique is relatively stable for beginners in hysteroscopic submucosal myomectomy.Beginners need to strictly grasp the indications in the first 20 surgeries, master the operation, quickly deal with emergencies, in order to better fully master the technology. -
Key words:
- submucosal myoma /
- hysteroscope /
- learning curve
-
表 1 2组病人一般资料比较(x±s)
分组 n 年龄/岁 肌瘤最大径/cm D-二聚体/(mg/L) 血红蛋白/(g/mL) 肌瘤分型 0型 Ⅰ型 Ⅱ型 A组 20 49.62±7.23 3.02±1.33 0.41±0.21 118.93±18.62 1(5) 11(55) 8(40) B组 46 49.34±9.35 3.02±1.01 0.38±0.16 118.13±18.59 3(6.5) 27(58.7) 16(34.8) t — 0.12 0.00 0.64 1.16 0.19△ P — >0.05 >0.05 >0.05 >0.05 >0.05 △示校正χ2值  下载: 导出CSV
下载: 导出CSV
表 2 2组病人手术相关指标比较(x±s)
分组 n 手术时间/min 术中出血量/mL 住院时间/d 术后并发症 血尿 发热 下肢深静脉血栓 低钾血症 A组 20 61.22±28.54 56.91±30.19 7.18±2.36 1 3 0 0 B组 46 37.14±17.18 16.90±14.49 6.02±1.40 0 2 1 1 t — 4.24 7.30 2.49 1.67△ P — < 0.01 < 0.01 < 0.05 >0.05 △示校正χ2值
下载: 导出CSV
表 3 2组病人术后恢复及随访指标比较(x±s)
分组 n 月经恢复时间/d 月经量/mL 血红蛋白浓度/(g/L) 术后随访妊娠 A组 20 28.46±12.11 46.46±29.87 129.33±18.86 1(5.00) B组 46 25.33±8.59 51.13±32.36 131.25±21.31 2(4.35) t — 1.20 0.55 0.35 — P — >0.05 >0.05 >0.05 >0.05△ △示Fisher′s确切概率法
下载: 导出CSV
-
[1] 张颖, 郭瑞霞. 宫腔镜下子宫肌瘤切除术的临床实践[J]. 实用妇产科杂志, 2019, 35(11): 805. [2] 管红娟. 宫腔镜手术治疗黏膜下子宫肌瘤的临床疗效及对患者月经量的影响[J]. 中国妇幼保健, 2020, 35(9): 1739. [3] 冯怡辰, 周君, 李少婧. 宫腔镜下子宫黏膜下肌瘤电切术的疗效和并发症[J]. 中国妇幼保健, 2016, 31(23): 4961. [4] 夏恩兰. 宫腔镜手术并发症诊治现状及展望[J]. 中国实用妇科与产科杂志, 2015, 31(5): 369. [5] 赵卫东, 周虎, 马杰, 等. 腹腔镜下复杂子宫肌瘤剔除术学习曲线研究[J]. 中国生育健康杂志, 2011, 22(5): 267. [6] 储云绵, 邱国同, 杜永星, 等. 73例胰腺节段切除术的学习曲线分析[J]. 中华肿瘤杂志, 2020, 42(12): 1020. [7] 白建萍, 周建政. 宫腔镜下黏膜下子宫肌瘤电切术影响妊娠的因素及对策[J]. 国际生殖健康/计划生育杂志, 2020, 39(2): 167. [8] LEE HJ, KIM JY, KIM SK, et al. Learning curve analysis and surgical outcomes of single-port laparoscopic myomectomy[J]. J Minim Invasive Gynecol, 2015, 22(4): 607. [9] 东洁, 徐维锋, 纪志刚. 单术者机器人辅助腹腔镜肾部分切除术的学习曲线[J]. 中华泌尿外科杂志, 2021, 42(4): 246. [10] 张亚坤, 门泉仓, 李霞霞, 等. 胸乳入路腔镜甲状腺手术学习曲线及经验体会[J]. 中国内镜杂志, 2020, 26(5): 48. -

 点击查看大图
点击查看大图
图(1)表(3)
计量
- 文章访问数: 1736
- HTML全文浏览量: 917
- PDF下载量: 3
- 被引次数: 0
