

-
股骨颈骨折以股骨头下至股骨颈基底部之间骨折为特征[1],老年人群股骨颈骨折的发病率高达146/10万,并呈持续增长趋势,可造成较高的致残率和病死率,严重威胁社会公共健康[2-3]。手术治疗是目前股骨颈骨折最有效的治疗方式,能够使病人尽早进行肢体活动和功能锻炼。而下肢深静脉血栓(lower extremity deep venous thrombosis, LDVT)是股骨颈骨折术后常见的并发症,一旦处理不当,可引起剧烈疼痛、股青肿甚至发生肺栓塞致使病人死亡[4]。由于LDVT的高发病率和高危害性[5],围手术期对LDVT的预防一直是骨科医生关注的热点,但关于个体化预测股骨颈骨折术后LDVT发生率的单项研究较少。本研究就骨股颈骨折术后发生LDVT的独立危险因素进行分析。现作报道。
-
回顾性分析2018年12月至2019年12月因股骨颈骨折于我院行手术治疗的老年病人的病历资料。入选标准:年龄≥60岁,性别不限;符合成人股骨颈骨折的诊断标准[6];ASA分级术前风险评估,能耐受手术且围手术期可进行常规的抗血栓预防方案;术前多普勒彩超检查双下肢未见血管性及血栓性疾病;临床资料完整。排除标准:合并恶性肿瘤;住院期间长期有活动性出血;肝、肾功能不全;伴有心脑血管疾病长期服用抗凝药物(如阿司匹林、氯吡格雷、华法林等)治疗。本次研究经医院伦理委员会审批通过。严密监测纳入病人的术后病情,观察病人有无出现患肢皮肤暗红、增粗、肿胀、疼痛、升温、呼吸困难等临床症状,以出现上述症状初步判断其为LDVT,并采用多普勒彩超予以进一步诊断,以结果显示深静脉管腔阻塞或充盈缺损改变确诊为并发LDVT[7]。
-
采集所有老年股骨颈骨折病人的临床病历、实验室资料及手术资料等,并做回顾性分析。具体纳入资料包括性别、年龄、体质量指数(BMI)、吸烟史、高血压、糖尿病、冠心病、D-二聚体、总胆固醇(TC)、三酰甘油(TG)、手术方式、手术时间、麻醉方式及手术等待时间。
-
采用χ2检验、logistic回归分析,并绘制ROC曲线。
-
共纳入143例老年股骨颈骨折病人,年龄60~88岁。术后发生LDVT有24例,发生率为16.78%,未发生LDVT有119例,分别设为LDVT组和非LDVT组。LDVT组病人均未出现肺栓塞症状和死亡病例。
-
2组病人性别、年龄、吸烟史、高血压、冠心病、D-二聚体、手术方式等因素差异均无统计学意义(P>0.05),而BMI、糖尿病、TC、TG、手术时间、麻醉方式及手术等待时间等差异均有统计学意义(P < 0.01)(见表 1)。
因素 LDVT组
(n=24)非LDVT组
(n=119)χ2 P 性别 男
女11
1367
520.88 >0.05 年龄/岁 60~ < 70
≥7014
1068
510.01 >0.05 BMI/(kg/m2) ≥24
< 2415
934
8510.21 < 0.01 吸烟史 是
否8
1636
830.09 >0.05 高血压 是
否6
1831
880.01 >0.05 糖尿病 是
否10
1417
1029.78 < 0.01 冠心病 是
否5
1933
860.49 >0.05 D-二聚体/(mg/L) >0.5
≤0.513
1142
773.01 >0.05 TC/(mmol/L) >5.69
≤5.6910
1418
1018.93 < 0.01 TG/(mmol/L) >1.8
≤1.811
1321
989.14 < 0.01 手术方式 闭合复位空心钉内固定术 4 29 人工股骨头置换术 15 73 1.07 >0.05 人工髋关节置换术 5 17 手术时间/min ≥60
< 6016
841
788.65 < 0.01 麻醉方式 静吸复合麻醉
腰硬联合麻醉12
1224
959.44 < 0.01 手术等待时间/d ≥5
< 513
1127
929.82 < 0.01 表 1 一般资料单因素分析(n)
-
以术后LDVT发生情况为因变量(并发=1,未发生=0),以单因素分析中有统计学意义的7个项目为自变量[BMI(≥24 kg/m2=1, < 24 kg/m2=0);糖尿病(是=1,否=0);TC(>5.69 mmol/L=1,≤5.69 mmol/L=0);TG(>1.8 mmol/L=1,≤1.8 mmol/L=0);手术时间(≥60 min=1, < 60 min=0);麻醉方式(静吸复合麻醉=1,腰硬联合麻醉=0);手术等待时间(≥5 d=1, < 5 d=0)],进行二分类logistic回归分析,结果表明BMI≥24 kg/m2、糖尿病、TC>5.69 mmol/L、TG>1.8 mmol/L、手术时间≥60 min、静吸复合麻醉及手术等待时间≥5 d是老年股骨颈骨折病人术后发生LDVT的独立危险因素(P < 0.05~P < 0.01)(见表 2)。
因素 B SE Waldχ2 P OR(95%CI) BMI 2.651 0.815 10.57 < 0.01 14.170(2.866~70.046) 糖尿病 3.131 0.903 12.01 < 0.01 22.888(3.896~134.475) TC 2.404 0.785 9.37 < 0.01 11.071(2.375~51.599) TG 1.970 0.766 6.62 < 0.05 7.167(1.598~32.145) 手术时间 1.911 0.762 6.29 < 0.05 6.763(1.518~30.123) 静吸复合麻醉 2.607 0.822 10.06 < 0.01 13.558(2.708~67.888) 手术等待时间 1.348 0.667 4.08 < 0.05 3.848(1.041~14.223) 常量 -7.618 1.458 27.30 < 0.01 — 表 2 术后LDVT多因素logistic回归分析
-
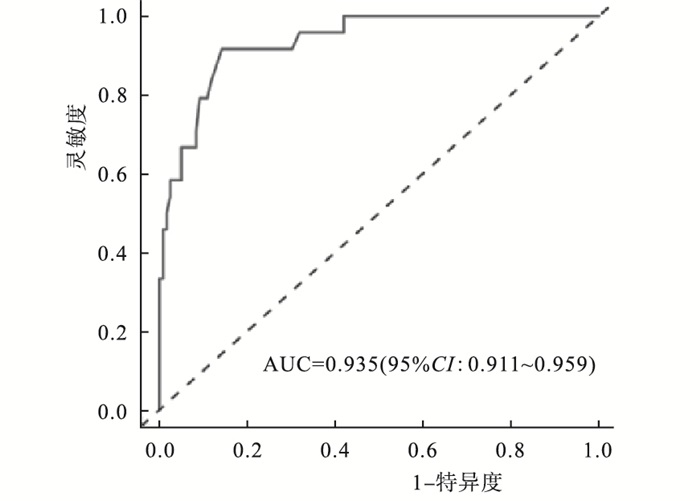
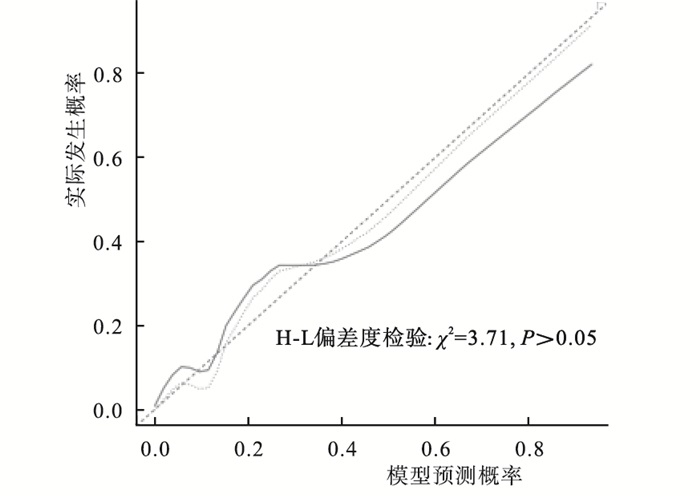
基于表 2中筛选出的独立危险因素,建立相关预测模型:LogitP =(BMI×14.170) +(糖尿病×22.888) +(TC×11.071) +(TG×7.167)+(手术时间×6.763)+(静吸复合麻醉×13.558)+(手术等待时间×3.848)-7.618。模型验证显示,偏差水平和区分度显示预测概率同实际发生概率差异无统计学意义(χ2=3.71,P>0.05)(见图 1)。一致性指数(C-index)指数0.935(95%CI:0.911~0.959)(见图 2),该预测模型具有良好的精准度和区分度。

图 1 模型预测老年股骨颈骨折病人术后发生LDVT风险的验证

图 2 模型预测老年股骨颈骨折病人术后发生LDVT的ROC曲线
-
老年人随着年龄的增长,骨质疏松患病率较高,股骨颈脆弱,防御能力较差,遭受轻微外力或跌倒时极易造成股骨颈骨折。病人主要表现为疼痛、肿胀、浅静脉曲张、全身反应等症状[8]。目前股骨颈骨折主要以手术治疗为主,但术后存在发生LDVT等诸多并发症的风险。本次研究纳入的143例老年股骨颈骨折病人,术后发生LDVT的有24例,发生率为16.78%,与LI等[9]报道中的19.5%相近。但与国内外关于股骨颈骨折术后LDVT发生率的报道悬殊较大[10-11],可能与样本均取自于单中心且样本量有限有关。
血栓的形成是多种因素综合作用的结果,其中最主要的为静脉损伤、血流缓慢和血液高凝状态三大因素[12]。国内外均报道股骨颈骨折术后LDVT的危险因素较多[13-14],本研究通过调取老年病人的临床资料并结合报道中公认的危险因子,较为全面地筛选出老年股骨颈骨折病人术后发生LDVT的独立危险因素:(1)BMI≥24kg/m2。BMI是与体内脂肪总量密切相关的指标,主要反映病人全身性超重和肥胖,BMI≥24 kg/m2显示病人处于高体质量的超重状态。病人肥胖可引起内源性凝血系统活化、纤溶活性降低、血小板易聚集黏附以及血液流变学异常,导致血液高凝状态,使血栓更易形成和发展[15]。(2)糖尿病。持续的高血糖状态可引起血管内皮细胞损伤,血小板在受损内皮细胞上黏附聚集,纤维蛋白原水平增加,造成纤溶-凝血系统平衡被打破,导致血液黏稠度增加,血液处于高凝状态,易诱发LDVT的形成[16]。(3)TC>5.69 mmol/L和TG>1.8 mmol/L。TC、TG偏高表明血脂异常增多,血液中过多的胆固醇和三酰甘油会沉积在血管壁上,过氧化脂质增加,长期可引起血管壁增厚,血管内皮细胞营养摄取紊乱,从而直接导致血管内膜和纤维层损伤,引起内源性凝血系统激活。同时,高血脂可引起血液中乳糜颗粒增多,导致病人血液黏稠度升高,血液流速减慢,更易堵塞病人血管形成血栓[17]。(4)手术时间≥60 min。股骨颈位于人体的髋部,髋部分布各种穿支血管和肌肉群,骨折手术过程中需要进行脱位关节、假体复位、牵拉周围软组织等操作,不可避免地对周围血管造成损伤,造成术中出血。手术时间越长造成血管内膜完整性破坏的概率越大,出血量越多,引起的防御性炎症反应越激烈,从而导致病人血液黏稠度增高更易诱发血栓[18]。(5)静吸复合麻醉。可能是由于硬膜外腔吸收部分局麻药,引起交感神经兴奋降低,使病人下肢血管扩张,血流量增多,适度减轻了手术引起的静脉血管血流缓慢、血液黏稠度升高的现象,从而降低了血栓的发生率,故采用静吸复合麻醉的病人相对腰硬联合麻醉而言发生LDVT的概率更高[19]。(6)手术等待时间≥5 d。病人发生骨折距手术的时间越长,卧床制动的时间也就越长,合并骨折本身的创伤刺激可导致血流速度变缓,血液高凝,易聚集成团从而诱发血栓[20]。
本研究根据筛选出的7项独立危险因素(BMI≥24 kg/m2、糖尿病、TC>5.69 mmol/L、TG>1.8 mmol/L、手术时间≥60 min、静吸复合麻醉及手术等待时间≥5 d)建立了老年股骨颈骨折病人术后发生LDVT预测模型,并经验证H-L偏差度检验结果为χ2=3.71,P>0.05,C-index指数0.904(95%CI:0.869~0.939),说明该模型具有良好的精准度和区分度。使用人员可根据老年股骨颈骨折病人各项危险指标情况,通过公式计算即可得出术后LDVT的预测发生率。护理人员可以此筛查出高风险病人并作好针对性的护理对策:(1)术后患肢护理。术后严密监测下肢皮肤温度、色泽、肿胀程度的变化,注意适度抬高并保持一定的高度,禁止剧烈运动以防刺激引起静脉痉挛、血流淤滞。(2)饮食护理。指导病人进食低脂、高纤维素、高蛋白、易消化的食物以保持大便通畅,促进术后的髋部恢复和避免排便困难引起腹内压升高而影响下肢静脉回流。(3)预防性抗凝治疗护理。对于LDVT预测概率较高的病人应及时行血流动力学检查,必要时遵医嘱采用低分子肝素钠、低分子右旋糖酐等抗凝药物进行预防。(4)心理护理。护理中重视病人情绪变化,建立良好的护患关系,主动向病人介绍LDVT的病因、治疗方案、预后和注意事项,尽量消除病人对术后并发症的担忧情绪,对于存在焦虑、恐惧情绪的病人要给予耐心的疏导和鼓励。
综上所述,BMI≥24 kg/m2、糖尿病、TC>5.69 mmol/L、TG>1.8 mmol/L、手术时间≥60 min、静吸复合麻醉及手术等待时间≥5 d是老年股骨颈骨折病人术后发生LDVT的独立危险因素,笔者建立的预测模型具有准确的预测能力和区分度,临床应用价值较高。
老年股骨颈骨折病人术后下肢深静脉血栓的危险因素分析
Analysis of the risk factors of postoperative lower extremity deep venous thrombosis in elderly patients with femoral neck fracture
-
摘要:
目的探讨老年股骨颈骨折病人术后发生下肢深静脉血栓(LDVT)的危险因素。 方法回顾性分析因股骨颈骨折行手术治疗的老年病人病历资料,分别使用单因素和logistic回归多因素分析术后发生LDVT的独立危险因素,并建立相关预测模型。 结果体质量指数≥24 kg/m2、糖尿病、总胆固醇>5.69 mmol/L、三酰甘油>1.8 mmol/L、手术时间≥60 min、静吸复合麻醉及手术等待时间≥5 d是老年股骨颈骨折病人术后发生LDVT的独立危险因素(P < 0.05~P < 0.01)。预测老年股骨颈骨折病人术后发生LDVT的模型验证结果显示,H-L偏差度检验结果为χ2=3.71,P>0.05,C-index指数为0.904(95%CI:0.869~0.939),说明列线图预测模型具有良好的精准度和区分度。 结论老年股骨颈骨折病人术后发生LDVT的独立危险因素显示,建立的预测模型具有准确的预测能力和区分度,临床应用价值较高。 Abstract:ObjectiveTo investigate the risk factors of lower extremity deep venous thrombosis(LDVT) in elderly patients with femoral neck fracture after operation. MethodsThe medical records of femoral neck fracture elderly patients treated with surgical treatment were retrospectively analyzed.The independent risk factors of postoperative LDVT were analyzed using the univariate and logistic regression analysis, and the correlation prediction model was established. ResultsThe body mass index ≥24 kg/m2, diabetes mellitus, total cholesterol(TC)>5.69 mmol/L, triacylglycerol(TG) >1.8 mmol/L, operation time ≥60 min, intravenous inhalation combined anesthesia and operation waiting time ≥5 d were the independent risk factor of postoperative LDVT in elderly patients with femoral neck fracture(P < 0.05 to P < 0.01).The results of model verification in predicting postoperative LDVT in elderly patients with femoral neck fracture showed that the results of H-L deviation test were χ2=3.71 and P>0.05, and the C-index was 0.904(95%CI: 0.869-0.939), which indicated that the prediction model of line chart had good accuracy and differentiation. ConclusionsThe independent risk factors of postoperative LDVT in elderly patients with femoral neck fracture.The prediction model has accurate prediction ability and differentiation, and high clinical application value. -
Key words:
- femoral neck fracture /
- elderly /
- lower extremity deep venous thrombosis
-
表 1 一般资料单因素分析(n)
因素 LDVT组
(n=24)非LDVT组
(n=119)χ2 P 性别 男
女11
1367
520.88 >0.05 年龄/岁 60~ < 70
≥7014
1068
510.01 >0.05 BMI/(kg/m2) ≥24
< 2415
934
8510.21 < 0.01 吸烟史 是
否8
1636
830.09 >0.05 高血压 是
否6
1831
880.01 >0.05 糖尿病 是
否10
1417
1029.78 < 0.01 冠心病 是
否5
1933
860.49 >0.05 D-二聚体/(mg/L) >0.5
≤0.513
1142
773.01 >0.05 TC/(mmol/L) >5.69
≤5.6910
1418
1018.93 < 0.01 TG/(mmol/L) >1.8
≤1.811
1321
989.14 < 0.01 手术方式 闭合复位空心钉内固定术 4 29 人工股骨头置换术 15 73 1.07 >0.05 人工髋关节置换术 5 17 手术时间/min ≥60
< 6016
841
788.65 < 0.01 麻醉方式 静吸复合麻醉
腰硬联合麻醉12
1224
959.44 < 0.01 手术等待时间/d ≥5
< 513
1127
929.82 < 0.01  下载: 导出CSV
下载: 导出CSV
表 2 术后LDVT多因素logistic回归分析
因素 B SE Waldχ2 P OR(95%CI) BMI 2.651 0.815 10.57 < 0.01 14.170(2.866~70.046) 糖尿病 3.131 0.903 12.01 < 0.01 22.888(3.896~134.475) TC 2.404 0.785 9.37 < 0.01 11.071(2.375~51.599) TG 1.970 0.766 6.62 < 0.05 7.167(1.598~32.145) 手术时间 1.911 0.762 6.29 < 0.05 6.763(1.518~30.123) 静吸复合麻醉 2.607 0.822 10.06 < 0.01 13.558(2.708~67.888) 手术等待时间 1.348 0.667 4.08 < 0.05 3.848(1.041~14.223) 常量 -7.618 1.458 27.30 < 0.01 —
下载: 导出CSV
-
[1] ZAJONZ D, BRAND A, LYCKE C, et al. Risk factors for early infection following hemiarthroplasty in elderly patients with a femoral neck fracture[J]. Eur J Trauma Emerg Surg, 2018, 45(2): 207. [2] 刘元标, 朱明跃. 老年髋部骨折康复进展[J]. 实用老年医学, 2018, 32(6): 509. [3] 许一凡, 陈美凯, 陈雪荣. 股骨颈骨折临床分型研究进展[J]. 中国骨与关节损伤杂志, 2019, 34(10): 1009. doi: 10.7531/j.issn.1672-9935.2019.10.001 [4] BUDNIK I, BRILL A. Immune factors in deep vein thrombosis initiation[J]. Trends Immunol, 2018, 39(8): 610. doi: 10.1016/j.it.2018.04.010 [5] MUSTAFA J, ASHER I, STHOEGER Z. Upper extremity deep vein thrombosis: symptoms, diagnosis, and treatment[J]. Isr Med Assoc J, 2018, 1(20): 53. [6] 中华医学会骨科学分会创伤骨科学组, 中国医师协会骨科医师分会创伤专家工作委员会. 成人股骨颈骨折诊治指南[J]. 中华创伤骨科杂志, 2018, 20(11): 921. doi: 10.3760/cma.j.issn.1671-7600.2018.11.001 [7] 侯玉芬, 刘政. 下肢深静脉血栓形成诊断及疗效标准(2015年修订稿)[J]. 中国中西医结合外科杂志, 2016, 22(5): 520. doi: 10.3969/j.issn.1007-6948.2016.05.032 [8] KYEONG S, SHIN JE, YANG KH, et al. Neural predisposing factors of postoperative delirium in elderly patients with femoral neck fracture[J]. Sci Rep, 2018, 8(1): 7602. doi: 10.1038/s41598-018-26030-2 [9] LI Q, DAI B, XU J, et al. Can patients with femoral neck fracture benefit from preoperative thromboprophylaxis: A prospective randomized controlled trial[J]. Medicine(Baltimore), 2017, 96(29): e7604. [10] 孙健平, 王鹏飞, 张堃, 等. 髋部骨折围手术期深静脉血栓发生的时间规律及转归的前瞻性研究[J]. 国际外科学杂志, 2018, 45(11): 731. doi: 10.3760/cma.j.issn.1673-4203.2018.11.003 [11] DURAND WM, GOODMAN AD, JOHNSON JP, et al. Assessment of 30-day mortality and complication rates associated with extended deep vein thrombosis prophylaxis following hip fracture surgery[J]. Injury, 2018, 49(6): 1141. doi: 10.1016/j.injury.2018.03.019 [12] 陈晶晶, 陆国平. 静脉血栓栓塞的识别和防治研究进展[J]. 中国小儿急救医学, 2019, 26(3): 224. doi: 10.3760/cma.j.issn.1673-4912.2019.03.014 [13] 王晨, 王鹏飞, 宋哲, 等. 股骨颈骨折术后发生下肢深静脉血栓的相关研究[J]. 国际外科学杂志, 2018, 45(7): 452. doi: 10.3760/cma.j.issn.1673-4203.2018.07.005 [14] NICHOLAS G, JOHNSTON K, GAUDELLI C, et al. The incidence of proximal deep vein thrombosis after elective hip arthroscopy: a prospective cohort study in low risk patients[J]. J Hip Preserv Surg, 2016, 3(4): 295. [15] 乔力松, 许小毛, 杨鹤, 等. 超重及肥胖肺栓塞患者临床特征及预后分析[J]. 中华结核和呼吸杂志, 2018, 41(11): 863. doi: 10.3760/cma.j.issn.1001-0939.2018.11.007 [16] BILORA F, CERESA M, MILAN M, et al. The impact of deep vein thrombosis on the risk of subsequent cardiovascular events. A 14-year follow-up study[J]. Int Angiol, 2016, 36(2): 156. [17] MORELLI VM, LIJFERING WM, ROSENDAAL FR, et al. Lipid levels and risk of recurrent venous thrombosis: Results from the MEGA follow-up study[J]. J Thromb Haemost, 2017, 15(4): 695. doi: 10.1111/jth.13640 [18] 饶婕, 张向宁. 妇科手术后深静脉血栓形成高危因素的临床分析[J]. 安徽医药, 2018, 22(4): 663. doi: 10.3969/j.issn.1009-6469.2018.04.022 [19] 顾伟, 徐丹, 董军, 等. 腰硬联合阻滞麻醉对老年人下肢骨折手术麻醉效果的研究[J]. 国际老年医学杂志, 2019, 40(5): 282. -

 点击查看大图
点击查看大图
图(2)表(2)
计量
- 文章访问数: 2009
- HTML全文浏览量: 935
- PDF下载量: 6
- 被引次数: 0
