






-
关节置换术中理想的手术位置和植入物的放置对于假体长期生存、患肢最佳功能恢复至关重要。临床传统人工全膝关节置换术(TKA)因术中复杂的髓内定位装置和过度依赖术者经验来确定所需截骨厚度和角度,容易产生一定的偏差,导致手术失败[1]。有研究[2]表明,传统手术装置对截骨角度的精确率仅为实际解剖的75%。病人膝关节重度畸形和有严重的骨量不足或缺损时,传统的TKA手术精确率又会大大降低,以致无法满足临床疗效的要求[3]。
目前,3D打印是一项日益成熟的技术,具有个性化的模型优势,已广泛应用于骨科实验模型的制作、辅助材料打印、植入物打印和关节手术打印等领域[4-5],它可以为关节置换术的病人提供个性化的专属器械和植入物,并能充分考虑到解剖变异和缺陷对疗效的影响[6],弥补了传统TKA定位不准、截骨偏差诸多方面的不足,从而显著提高手术截骨的准确性、假体的机械强度和重建后膝关节的稳定性[7-9]。本次研究旨在进一步探析3D打印个性化截骨导板辅助TKA和传统TKA应用效果差异,为临床诊治复杂膝内翻畸形骨关节疾病提供理论参考。
-
病例来源于2018年1月至2020年8月于山东省文登整骨医院关节科经检查明确诊断为膝内翻畸形并骨性关节炎的病人。本次研究获得山东省文登整骨医院医学伦理委员会批准(伦理审批编号:NO.2017-013)。共42例(44膝)病人纳入研究对象,男17例,女25例;年龄62~75岁;左膝23例,右膝21例;X线提示均存在不同程度的内翻畸形,其中内翻≥20° 4膝,>10°~<20° 18膝,≤10° 22膝。为避免选择偏倚,由专人采用随机数字表法纳入分组,分为传统手术组和3D打印导板组。3D打印导板组21例(23膝)在3D打印截骨导板辅助下行TKA,传统手术组21例(21膝)接受传统TKA手术治疗。
-
采用骨关节炎诊疗指南(2018年版)诊断标准[10]:(1)近1个月内反复膝关节疼痛;(2)X线片(站立位或负重位)示关节间隙变窄,软骨下骨硬化和/或囊性变,关节边缘骨赘形成;(3)年龄≥50岁;(4)晨僵时间≤30 min;(5)活动时有骨擦音(感)。
-
(1) 符合上述诊断标准;(2)年龄60~79岁;(3)终末期严重膝内翻骨性关节炎者,内翻角度≥20°;(4)近半年内未行关节腔注射药物治疗;(5)所有病人及家属充分知情此项临床研究程序并签署知情同意书。
-
(1) 行膝关节翻修;(2)有严重心脑血管或肝肾功能不全等自身基础疾病多且复杂;(3)急性或慢性化脓性膝关节感染;(4)患肢神经血管有损伤;(5)无法判断疗效或资料不全;(6)术后不能积极配合治疗。
-
3D打印导板组:术前完善相关常规检查,行双下肢全长正位X线片检查以及膝关节三维CT检查。将获得的资料导入进行导板设计,打印膝关节解剖模型和截骨导板实体,并进行术前手术模拟。手术均采用膝前正中纵行切口、髌旁内侧入路,依次切开皮肤、皮下组织、深筋膜,沿髌骨内侧缘切开内侧支持带,沿股四头肌肌腱向近端延伸支持带切口,沿髌腱内缘向下切开至胫骨前内侧面。将髌骨向外翻转。屈膝90°,切除部分髌下脂肪垫、前交叉韧带、内外侧半月板前角。术中将3D打印的膝关节模型与病人膝关节进行匹配,确定解剖结构之后,安装3D股骨远端截骨导板,确保定位模块紧贴于膝关节解剖结构后进行截骨。胫骨近端截骨在安装3D胫骨截骨导板并与胫骨近端解剖结构匹配固定后完成截骨。重新检查病人的软组织平衡,适度调整后脉冲枪冲洗。根据假体型号安装假体并用骨水泥固定,检查力线以确保有良好的下肢力线。留置引流管一根,逐层关闭切口。传统手术组:手术暴露视野方法同3D打印导板组。于股骨髁间窝中点钻孔,插入股骨髓内定位导向杆行股骨远端截骨,用髓外定位器沿胫骨外侧平台下截骨。余后操作同3D打印导板组。2组均在即将关闭切口时注入氨甲环酸100 mL, 术后抗生素、抗凝药物治疗,监测24 h引流量并拔除引流管。所有手术均在硬膜外麻醉下进行,由同一位资深骨科主刀医生操作,同一组医生参与完成。术中不置换髌骨,均使用国产北京春立品牌同一类型的表面膝关节假体。由专业康复治疗人员指导病人进行术后功能锻炼。
-
(1) 记录2组病人的手术时间、术中失血量、术后24 h引流量;(2)影像学测量术后股骨与胫骨机械轴夹角(aMFTA)即下肢力线情况;(3)美国膝关节协会评分(American knee society knee score,KSS评分)[11]:85~100分为优,70~84分为良,60~69分为可,60分以下为差;(4)WOMAC评分[12]:指数越高,患膝功能越差,代表疗效越差。
-
采用t检验、χ2检验和方差分析。
-
2组病人的年龄、性别和膝内翻患侧差异均无统计学意义(P>0.05)(见表 1),具有可比性。
分组 n 年龄(x±s)/岁 男 女 患侧 左 右 3D打印导板组 23 63.70±4.00 8 13 13 10 传统手术组 21 63.80±4.56 9 12 10 11 χ2 — 0.19* 0.10 0.35 P — >0.05 >0.05 >0.05 *示t值 表 1 2组病人一般资料的比较
-
所有病均人成功实施手术,术后24 h拔除引流管,术后1周能自主功能锻炼并在辅助器下行走锻炼,切口甲级愈合,均未发生感染、神经血管损伤及假体松动移位等并发症,术后6个月顺利随访。
-
与传统手术组病人比较,3D打印导板组手术时间显著缩短,术中失血量显著减少,术后24 h引流量显著减少,差异均有统计学意义(P<0.01)(见表 2)。
分组 n 手术时间/min 术中失血量/mL 术后24 h引流量/mL aMFTA/(°) 3D打印导板组 23 75.52±6.39 150.70±8.54 232.61±10.43 2.33±0.28 传统手术组 21 94.90±4.33 207.33±9.48 303.05±12.05 1.81±0.21 t — 11.66 20.85 20.78 7.03 P — < 0.01 < 0.01 < 0.01 < 0.01 表 2 2组围手术期相关指标比较(x±s)
-
术后,3D打印导板组与传统手术组相比,aMFTA明显减小(P<0.01)(见表 2)。
-
2组病人术后6个月KSS临床及功能评分均明显高于术前(P<0.01)。术前, 2组病人KSS临床评分及功能评分比较,差异均无统计学意义(P>0.05);术后6个月,2组病人KSS临床评分比较,差异无统计学意义(P>0.05),3D打印导板组功能评分高于传统手术组(P<0.05)(见表 3)。
分组 n KSS临床评分 KSS功能评分 术前 3D打印导板组 23 53.17±3.07 52.96±3.20 传统手术组 21 53.43±3.11 53.14±2.87 t — 0.27 0.20 P — >0.05 >0.05 术后 3D打印导板组 23 86.30±2.12** 88.00±1.73** 传统手术组 21 86.05±1.36** 86.71±1.82** t — 0.47 2.40 P — >0.05 < 0.05 注:与术前比较**P<0.01 表 3 2组病人术前及术后6个月KSS评分比较(x±s;分)
-
2组病人术后3个月和术后6个月WOMAC评分较术前均随着时间的增加而降低(P<0.01);组间比较显示,术前、术后6个月2组间WOMAC评分差异均无统计学意义(P>0.05),术后3个月时3D打印导板组评分低于传统手术组(P<0.05)(见表 4)。
分组 术前 术后3个月 术后6个月 F P MS组内 3D打印导板组 74.48±6.09 18.00±2.07** 11.61±1.47**△△ 1 268.15 < 0.01 14.502 传统手术组 73.29±6.57 20.10±3.21** 11.57±1.43**△△ 1 898.58 < 0.01 18.522 t 0.63 2.55 0.09 — — — P >0.05 < 0.05 >0.05 — — — q检验:与术前比较**P<0.01;与术后3个月比较△△P<0.01 表 4 2组病人WOMAC评分比较(x±s;分)
-
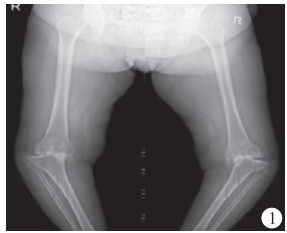
病人,女,63岁,双膝关节肿痛、畸形伴功能障碍20年。左膝屈曲5°~85°,内翻30°;右膝屈曲5°~90°,内翻25°。X线片示:双膝关节边缘骨质增生,内侧关节间隙显著变窄,关节面硬化破碎不平,内见低密度囊区,膝关节内缘见游离体,双膝关节对应欠佳,呈半脱位征象。右股骨远端类圆形高密度影,左胫骨近端低密度囊区。术前讨论认为病人膝关节内翻畸形严重,胫骨平台内侧缺损大,外侧副韧带松弛,内侧副韧带紧缩,常规膝关节假体软组织平衡困难,需要在3D打印截骨导板技术辅助下行TKA,考虑左侧膝关节内翻畸形程度更大,先行左侧TKA,11个月后行右侧TKA(见图 1~8)。

图 1 术前下肢全长正位片

图 2 左TKA术后下肢全长正位片, 经测量下肢力线良好

图 3 3D打印的截骨导板

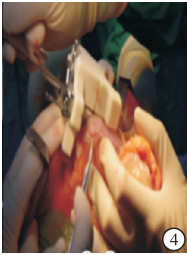
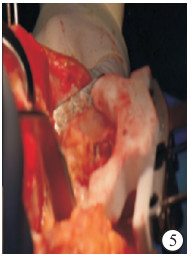
图 4 术中使用截骨导板对股骨、胫骨进行截骨

图 5 术中使用截骨导板对股骨、胫骨进行截骨

图 6 双膝关节置换术后正位片, 显示人工假体位置植人良好

图 7 术前病人站立位图,双膝关节呈重度屈曲内翻畸形,需在辅助行走器下行走

图 8 双膝关节使用3D打印截骨导板辅助行TKA后站立位图, 显示双下肢矫形良好
-
骨关节炎是使老年人致残最常见的疾病之一,与性别、年龄、体质量指数、下肢机械轴、生物力学等因素有关[13-15]。其病变部位主要在具有承重作用的髋、膝、踝关节,其中膝关节发病率最高,临床表现为软骨和软骨下骨的退变和磨损[16-17]。由于正常人的下肢呈轻度内翻,导致内侧间隙负荷大最易受累,所以膝内翻畸形是临床常见的类型。TKA是治疗膝内翻畸形并骨关节炎最有效的方式,具有减轻病人疼痛、矫正畸形、恢复下肢力线、重建关节功能的作用,从而提高病人的生活质量。随着老龄化的日益加剧,人们对TKA的需求量显著增加。有研究[18]表明接受TKA的病人存活率约为95%。同时据报道[19],近19%的病人对TKA术后仍不满意,这可能与术后疼痛、感染、传统TKA截骨角度偏差导致的假体不稳定以及假体植入的精准性等密切相关,特别是对于复杂膝内翻畸形的TKA,矫正畸形、恢复下肢力线的难度大,此时需要采用更加精准的手术方法。3D打印技术辅助TKA因其操作简单、个性化模型、截骨精准、畸形矫正程度大的优势广受青睐。3D打印在术前能够更好地显示完整的3D解剖结构,并根据CT图像对截骨量进行数字化规划,从而提高了复杂高难度的严重关节畸形和严重软组织挛缩病人术前方案规划的准确性、手术植入的精确性和安全性,并减少了术后神经、血管等并发症发生[17, 20-21]。
结合前人的研究[22-25],本次研究同样认为相比于传统的TKA,3D打印截骨导板辅助TKA手术时间相对较短,这与术中不需要常规应用髓内和髓外定位装置反复测量力线和截骨角度,也不需要反复旋转股骨来测量假体试模与关节匹配程度,以及手术操作相对简单有关。有研究表明缩短手术时间的潜在的临床优势与低感染率相关[26-27],同时也减少了病人隐性失血量,降低了手术风险[28-29]。此外研究也发现3D打印截骨导板辅助TKA可显著减少术中及术后的失血量,可能的原因有:(1)手术中使用个性化截骨导航模板精确定位,导向器与病人完美匹配,无需反复校正,从而减少了对骨皮质血管的损伤;(2)髓内导向杆装置进入股骨髓腔较浅,没有损伤髓内松质骨和髓内血管,减少了髓腔内的出血量;(3)术中降低了试模时反复屈伸膝关节对周围软组织的剥离程度。相关研究[30-31]指出由于术中没有股骨髓内定位杆的挤压,同时降低了发生脂肪栓塞的风险。传统TKA入髓杆插入股骨干髓腔很深,增加了手术对人体的创伤程度。3D打印截骨导板辅助TKA可以精准定位入髓位置且深度较浅,显著提高了精准性的同时也大大提高了手术的安全性。由此可见,3D打印截骨导板辅助TKA手术方法优越之处符合现代临床追求的微创精准理念。
术中精准截骨重建下肢机械轴力线和实现假体旋转轴线的精准定位是TKA手术成功和术后肢体功能恢复的两个必要条件[32-33]。良好的下肢力线对于TKA长期疗效及降低植入物翻修率有极其重要的意义[34]。本次研究得出的结论中,传统的TKA中aMFTA总体大于3D打印导板辅助下行TKA,说明使用3D打印导板辅助下行TKA能够减小下肢力线误差,恢复下肢机械轴力线的精确度更理想。在旋转对线方面,股骨假体旋转轴线的良好定位是实现关节稳定和减少术后并发症发生的首要因素[35],同时与人工关节的生存率息息相关[36]。孙茂淋等[37]研究发现3D个性化引导技术可以改善术后步态参数,具体体现在摆动期膝关节最大屈曲角度,还可以帮助重建更准确的髌骨轨迹和全膝关节置换术中的旋转对齐,避免过度或不足扭转的发生。KSS评分是膝关节功能恢复的重要评价指标之一,所有病人术后6个月与术前相比关节灵活性显著提高、痛苦明显减轻,但术后KSS功能评分3D打印截骨导板辅组优于传统TKA组,提示3D打印截骨导板行TKA对改善病人膝关节功能疗效更优,这与近年来研究[38-39]结果报道相符合。在WOMAC评分比较中,术后3个月3D打印截骨导板组优于传统TKA组,说明3D打印辅助TKA对于术后功能更快地恢复具有积极的临床应用价值。
综上所述,3D打印截骨导板辅助TKA有很多优势,更适用于膝关节严重畸形、高龄且基础状态差、创伤耐受度低的骨关节炎人群。但其也存在不足之处。首先,术前的导板设计制作和手术模拟需要耗费一定的时间;其次,需要拍摄下肢的CT,除了给病人增加经济负担外,所带来的辐射与X线相当;最后,由于重度膝内翻畸形的病人伴有不同程度的软组织失衡,而术前规划均只针对骨性结构,无法对软组织环境进行架构,在实际手术中需要术者进行综合考量、精确判断,若截骨后无法获得软组织挛缩松解平衡,则不必拘于术前规划而进行截骨量的调整,从而取得理性的效果。尽管3D打印目前尚存在一些缺点,但因其个性化组织工程支架材料以及假体植入物的制造等优点,在未来关节外科修复重建领域的发展中必将起到至关重要的作用。
3D打印截骨导板辅助人工全膝关节置换术在重度膝内翻畸形中的应用观察
Application value of 3D printed osteotomy guide plate assisted artificial total knee arthroplasty in severe genu varus deformity
-
摘要:
目的探析3D打印截骨导板技术辅助人工全膝关节置换术(TKA)在重度膝内翻畸形骨性关节炎中的应用,提高临床TKA的精准性。 方法收集42名重度膝关节内翻畸形病人的临床资料进行分析。将病人采取随机数字表法分为2组,其中3D打印导板组21例(23膝)在3D打印截骨导板辅助下行TKA,传统手术组21例(21膝)接受传统TKA手术治疗。记录2组病人的手术时间、术中失血量、术后24 h引流量、术后股骨与胫骨机械轴夹角(aMFTA)以及膝关节KSS、WOMAC评分并进行统计分析。 结果所有病人均成功实施手术并进行6个月随访。与传统手术组比较,3D打印导板组手术时间显著缩短(P<0.01),术中失血量、术后24 h引流量均明显减少(P<0.01);术后aMFTA低于传统手术组(P<0.01)。2组病人术后6个月KSS临床及功能评分均明显高于术前(P<0.01), 术后6个月3D打印导板组KSS功能评分高于传统手术组(P<0.05), 而2组KSS临床评分差异无统计学意义(P>0.05)。2组病人术后3个月和术后6个月WOMAC评分较术前均随着时间的增加而降低(P<0.01);术后3个月,3D打印导板组评分低于传统手术组(P<0.05)。2组病人术后均未出现感染、神经损伤、深静脉血栓形成、假体松动脱位等并发症。 结论3D打印截骨导板技术辅助TKA治疗膝关节重度内翻畸形较传统TKA手术兼备时间短、失血量少、手术截骨精准度提高和术后功能恢复快的优点,临床疗效更佳。 Abstract:ObjectiveTo investigate the application value of 3D printing osteotomy technology assisted artificial total knee arthroplasty(TKA) in severe genu varus deformity to improve the accuracy of clinical TKA. MethodsThe clinical data of 42 patients with severe genu varus deformity were collected and analyzed.The patients were divided into two groups by random number table method.The 3D printing guide group(21 cases, 23 knees) were treated with 3D printed osteotomy guide plate assisted TKA, and the traditional surgical group were treated with traditional TKA.The operative time, intraoperative blood loss, 24 hours postoperative drainage, postoperative femoral and tibial mechanical shaft clamping angle(aMFTA) and knee joint KSS and WOMAC scores were recorded and statistically analyzed. ResultsAll patients were successfully operated and followed up for 6 months.Compared with the traditional surgery group, the operation time was significantly shortened(P<0.01), and the intraoperative blood loss and 24 hours postoperative drainage volume were significantly reduced in the 3D printing guide group(P<0.01).The postoperative aMFTA in 3D printing guide group was lower than that in traditional surgery group(P<0.01).After 6 months of surgery, the clinical and functional scores of KSS in two groups were significantly higher than those before surgery(P<0.01), the functional score of KSS in 3D printing guide group was higher than that in traditional surgery group(P<0.05), but there was no statistical significance in the clinical score of KSS between two groups(P>0.05).Compared with that before surgery, the WOMAC scores in two groups after 3 and 6 months of surgery decreased with the increase of time(P<0.01).After 3 months of surgery, the score of 3D printing guide group was lower than that of the traditional surgery group (P<0.05).No postoperative complications such as infection, nerve injury, deep vein thrombosis, prosthesis loosening and dislocation occurred in two groups. ConclusionsCompared with the traditional TKA surgery, the 3D printed osteotomy guide plate technology in the treatment of severe genu varus deformity has the advantages of shorter operation time, less blood loss, effective improving the surgical osteotomy accuracy, quick recovering the postoperative function and better clinical effects. -
Key words:
- total knee arthroplasty /
- 3D printing /
- knee genu varus /
- osteoarthritis
-
表 1 2组病人一般资料的比较
分组 n 年龄(x±s)/岁 男 女 患侧 左 右 3D打印导板组 23 63.70±4.00 8 13 13 10 传统手术组 21 63.80±4.56 9 12 10 11 χ2 — 0.19* 0.10 0.35 P — >0.05 >0.05 >0.05 *示t值  下载: 导出CSV
下载: 导出CSV
表 2 2组围手术期相关指标比较(x±s)
分组 n 手术时间/min 术中失血量/mL 术后24 h引流量/mL aMFTA/(°) 3D打印导板组 23 75.52±6.39 150.70±8.54 232.61±10.43 2.33±0.28 传统手术组 21 94.90±4.33 207.33±9.48 303.05±12.05 1.81±0.21 t — 11.66 20.85 20.78 7.03 P — < 0.01 < 0.01 < 0.01 < 0.01
下载: 导出CSV
表 3 2组病人术前及术后6个月KSS评分比较(x±s;分)
分组 n KSS临床评分 KSS功能评分 术前 3D打印导板组 23 53.17±3.07 52.96±3.20 传统手术组 21 53.43±3.11 53.14±2.87 t — 0.27 0.20 P — >0.05 >0.05 术后 3D打印导板组 23 86.30±2.12** 88.00±1.73** 传统手术组 21 86.05±1.36** 86.71±1.82** t — 0.47 2.40 P — >0.05 < 0.05 注:与术前比较**P<0.01
下载: 导出CSV
表 4 2组病人WOMAC评分比较(x±s;分)
分组 术前 术后3个月 术后6个月 F P MS组内 3D打印导板组 74.48±6.09 18.00±2.07** 11.61±1.47**△△ 1 268.15 < 0.01 14.502 传统手术组 73.29±6.57 20.10±3.21** 11.57±1.43**△△ 1 898.58 < 0.01 18.522 t 0.63 2.55 0.09 — — — P >0.05 < 0.05 >0.05 — — — q检验:与术前比较**P<0.01;与术后3个月比较△△P<0.01
下载: 导出CSV
-
[1] SCHIRALDI M, BONZANINI G, CHIRILLO D, et al. Mechanical and kinematic alignment in total knee arthroplasty[J]. Ann Transl Med, 2016, 4(7): 130. doi: 10.21037/atm.2016.03.31 [2] PARK A, NAM D, FRIEDMAN MV, et al. Inter-observer precision and physiologic variability of MRI land-marks used to determine rotational alignment in conventional and patient-specific TKA[J]. J Arthroplasty, 2015, 30(2): 290. doi: 10.1016/j.arth.2014.08.015 [3] SHEN ZM, WANG H, DUAN YQ, et al. Application of 3D printed osteotomy guide plate-assisted total knee arthroplasty in treatment of valgus knee deformity[J]. J Orthop Surg Res, 2019, 14(1): 327. doi: 10.1186/s13018-019-1349-9 [4] MA LM, ZHOU Y, ZHU Y, et al. 3D printed guiding templates for improved osteosarcoma resection[J]. Sci Rep, 2016, 6: 23335. doi: 10.1038/srep23335 [5] WOON JTK, ZENG I, CALLIESS T, et al. Outcome of kinematic alignment using patient-specific instrumentation versus mechanical alignment in TKA: a meta-analysis and subgroup analysis of randomised trials[J]. Arch Orthop Trauma Surg, 2018, 138(9): 1293. doi: 10.1007/s00402-018-2988-8 [6] KUMAR P, VATSYA P, RAJNISA RK, et al. Application of 3D Printing in hip and knee arthroplasty: a narrative review[J]. Indian J Orthop, 2020, 55(1): 14. [7] LI HK, Yao Q, SHEN B, et al. Application of 3D printing technology to left atrial appendage occlusion[J]. Int J Cardiol, 2017, 231: 258. doi: 10.1016/j.ijcard.2017.01.031 [8] YOU W, LIU LJ, CHEN HX, et al. Application of 3D printing technology on the treatment of complex proximal humeral fractures (Neer3-part and 4-part) in old people[J]. Orthop Traumatol Surg Res, 2016, 102(7): 897. doi: 10.1016/j.otsr.2016.06.009 [9] WANG FP, ZHU J, PENG XJ, et al. The application of 3D printed surgical guides in resection and reconstruction of malignant bone tumort[J]. Oncol Lett, 2017, 14(4): 4581. doi: 10.3892/ol.2017.6749 [10] 中华医学会骨科学分会关节外科学组. 骨关节炎诊疗指南(2018年版)[J]. 中华骨科杂志, 2018, 38(12): 705. doi: 10.3760/cma.j.issn.0253-2352.2018.12.001 [11] 裴福兴, 陈安民. 骨科学[M]. 北京: 人民卫生出版社, 2016: 102. [12] 岳恒, 甄平, 梁小弟. 低强度聚焦超声与低强度脉冲超声治疗轻度创伤性膝骨关节炎: 疼痛与功能的差异[J]. 中国组织工程研究, 2021, 25(26): 4101. doi: 10.12307/2021.105 [13] LIU RX, YUAN XL, YU J, et al. An updated meta-analysis of the asporin gene D-repeat in knee osteoarthritis: effects of gender and ethnicity[J]. J Orthop Surg Res, 2017, 12(1): 148. doi: 10.1186/s13018-017-0647-3 [14] LAW RJ, NAFEES S, HISCOCK J, et al. A lifestyle management programme focused on exercise, diet and physiotherapy support for patients with hip or knee osteoarthritis and a body mass index over 35: a qualitative study[J]. Musculoskeletal Care, 2019, 17(1): 145. doi: 10.1002/msc.1382 [15] JESU'S CL, ARACELI OR, IRENE TS, et al. Association between the functional impact of osteoarthritis and body mass index in women[J]. Rev Med Chil, 2018, 146(9): 987. doi: 10.4067/s0034-98872018000900987 [16] THOMAS FB, MARIA N, SOFIA MS, et al. Causal factors of knee, hip and hand osteoarthritis: a Mendelian randomization study in the UK Biobank[J]. Arthritis Rheumatol, 2019, 71(10): 1634. doi: 10.1002/art.40928 [17] KHLOPAS H, KHLOPAS A, SAMUEL LT, et al. Current concepts in osteoarthritis of the ankle: review[J]. Surg Technol Int, 2019, 35: 280. [18] 林海滨, 黄文华, 陈宣煌, 等. 基于3D打印和接骨板标准件库数字化的股骨远端骨折内固定[J]. 中华医学杂志, 2016, 96(5): 344. doi: 10.3760/cma.j.issn.0376-2491.2016.05.006 [19] MANNAN A, SMITH TO. Favourable rotational alignment outcomes in PSI knee arthroplasty: a level 1 systematic review and meta-analysis[J]. Knee, 2016, 23(2): 186. doi: 10.1016/j.knee.2015.08.006 [20] HOEKSTRA H, ROSSEELS W, SERMON A, ea al. Corrective limb osteotomy using patient specific 3D-printed guides: a technical note[J]. Injury, 2016, 47(10): 2375. doi: 10.1016/j.injury.2016.07.021 [21] QIU B, LIU F, TANG BS, et al. Clinical study of 3D imaging and 3D printing technique for patient-specific instrumentation in total knee arthroplasty[J]. J Knee Surg, 2017, 30(8): 822. doi: 10.1055/s-0036-1597980 [22] LI B, LEI P, LIU H, et al. Clinical value of 3D printing guide plate in core decompression plus porous bioceramics rod placement for the treatment of early osteonecrosis of the femoral head[J]. J Orthop Surg Res, 2018, 13(1): 130. doi: 10.1186/s13018-018-0812-3 [23] WU QP, YU T, LEI B, et al. A new individualized three-dimensional printed template for lateral ankle ligament reconstruction[J]. Med Sci Monit, 2020, 26: e922925. [24] CHEN GY, HAN Q, LIU H, et al. Accurate osteotomy for the treatment of a rare case of postaxial polydactyly of the foot that originated from a deformed calcaneus using a 3d-printed guiding plate[J]. J Foot Ankle Surg, 2019, 58(1): 171. doi: 10.1053/j.jfas.2018.07.003 [25] 王玄, 于卓力, 纪楠, 等. 3D打印个性化截骨导板与传统截骨方法在全膝关节置换中的应用与比较[J]. 中国组织工程研究, 2018, 22(19): 3049. doi: 10.3969/j.issn.2095-4344.0305 [26] 郭飞, 王全鹏, 代建昊, 等. CT三维重建配合3D打印技术在辅助寰枢椎椎弓根螺钉置入的应用价值评估[J]. 蚌埠医学院学报, 2018, 43(6): 784. [27] 张述东, 李世盛. 基于3D打印技术的个性化导航模板应用于全膝关节置换术中的临床价值[J]. 中国骨与关节杂志, 2021, 10(1): 61. doi: 10.3969/j.issn.2095-252X.2021.01.012 [28] 邬波, 柳椰, 马旭, 等. 3D打印个性化导航模板在全膝关节置换术中的应用[J]. 中国骨与关节损伤杂志, 2017, 32(2): 148. [29] 张衡, 刘扬, 官建中, 等. 3D打印技术在桡骨远端不稳定性骨折微创治疗中的应用[J]. 蚌埠医学院学报, 2019, 44(4): 437. doi: 10.13898/j.cnki.issn.1000-2200.2019.04.005 [30] 陈拥, 王增辉, 朴成哲. 3D打印个性化截骨导板辅助行全膝关节置换的应用[J]. 中国组织工程研究, 2019, 23(8): 1155. [31] CHAN WC, PINDER E, LOEFFLER M. Patient-specific instrumentation versus conventional instrumentation in total knee arthroplasty[J]. J Orthop Surg (Hong Kong), 2016, 24(2): 175. doi: 10.1177/1602400211 [32] 杨滨, 袁亮, 张克, 等. 新型改良3D打印个体化导向器辅助全膝关节置换术的精准度研究[J]. 中华骨科杂志, 2021, 41(2): 67. doi: 10.3760/cma.j.cn121113-20200715-00451 [33] 邱冰, 张明娇, 唐本森, 等. 基于3D打印个性化手术导航模板辅助下的人工全膝关节置换[J]. 中国组织工程研究, 2015, 19(48): 7731. doi: 10.3969/j.issn.2095-4344.2015.48.004 [34] CERQUIGLINI A, HENCKEL J, HOTHI H, et al. 3D patient imaging and retrieval analysis help understand the clinical importance of rotation in knee replacement[J]. Knee Surg Sports Traumatol Arthrosc, 2018, 26(11): 3351. [35] LEE SS, LEE YI, KIM DU, et al. Factors affecting femoral rotational angle based on the posterior condylar axis in gapbased navigation assisted total knee arthroplasty for valgus knee[J]. PLoS One, 2018, 13(5): e197335. [36] 方亮, 董睿. 3D打印个体化器械操作在全膝关节置换术中的应用现状[J]. 中国骨伤, 2019, 32(6): 582. [37] 孙茂淋, 杨柳, 何锐, 等. 3D打印导板辅助人工全膝关节置换术后患者步态分析[J]. 中国修复重建外科杂志, 2019, 33(8): 953. [38] 黄辰宇, 唐成, 魏波, 等. 3D打印手术导板在膝关节内外翻畸形患者全膝关节置换中的应用[J]. 中国组织工程研究, 2021, 25(18): 2789. [39] 李杨, 田华, 耿霄. 计算机导航系统、3D打印截骨导板与传统器械对全膝关节置换术手术时间和下肢力线恢复的影响[J]. 中华医学杂志, 2018, 14(2): 2157. -

 点击查看大图
点击查看大图
图(8)表(4)
计量
- 文章访问数: 3078
- HTML全文浏览量: 1688
- PDF下载量: 7
- 被引次数: 0
