

-
创伤性颅脑损伤(traumatic brain injury,TBI)是当今世界一个重要的公共卫生问题,TBI的发生率约为5 000万人次/年[1]。TBI后,病人常常遗留有不同程度的神经功能障碍,给家庭和社会带来了沉重的负担[2]。其中,认知功能障碍(如注意障碍)是TBI病人伤后长期存在的后遗症之一。研究[3-5]表明,认知功能依赖于人脑中大规模分布式神经网络的集成运行,其中默认网络(default mode network, DMN)被认为是注意任务匹配的神经网络,DMN是一个大脑系统, 它包含一些功能联系紧密的脑区,如扣带回/前楔叶、顶下小叶,内侧前额叶及特定纤维束(胼胝体膝部、扣带束、额枕上束)。磁共振弥散张量成像技术(diffusion tensor imaging, DTI)是根据水分子移动观察和追踪脑白质纤维束的非侵入性检查方法[6-8]。本研究采用临床常用的DTI技术对TBI病人的白质纤维束进行评估,同时采用认知功能量表分析TBI病人的注意障碍。以期揭示TBI后神经纤维的断裂可造成DMN的变化,且急性期DMN的改变与TBI病人注意障碍具有一定的相关性,为TBI病人早期注意障碍的评估和检测提供客观依据。
-
选择2018-2019年淮北矿工总医院集团神经外科收治的符合纳入标准的TBI病人。纳入标准: (1)年龄18~80岁; (2)依据现病史及CT确诊的TBI病人; (3)TBI病人临床资料及DTI检查资料完整; (4)所有病人均无手术指征,均采用保守药物治疗。排除标准:(1)既往有过脑外伤史; (2)伴有其他严重心脑血管疾病的、重要脏器严重功能障碍的病人; (3)妊娠或哺乳期妇女;(4)精神病病人,包括药物和酒精滥用史和智力发育迟钝史; (5)存在理解和认知功能障碍的病人; (6)存在语言功能障碍病人; (7)不愿参与本次研究的病人。TBI病人45例,其中男24例,女21例,年龄18~75岁。招募30名健康志愿者作为对照组,其中男16名,女14名,年龄19~67岁。所有入选者均签署知情同意书。
-
所有TBI病人均在急诊行头颅CT检查,且在TBI急性期行磁共振及DTI检查。将DTI序列图像导入工作站,并进行后处理,产生纤维束示踪成像图、表观弥散系数(apparent diffusion coefficient, ADC)图及各项异性分数(fractional anisotropy, FA)图。选取默认网络相关脑区或纤维束,主要包括扣带束(Cing)、胼胝体膝部(gCC)、额枕上束(SFOF)。将选取的感兴趣区域经软件处理生成纤维束图,并测量相应FA和ADC值。
-
依据相关文献[9]报道,使用Stroop色词量表Victoria版本(VST)对本项目中TBI病人进行评测。VST主要包括以下内容:文字(W部分)、圆点(D部分)及颜色(C部分)。在D部分所示圆点颜色中,受试者需要以最快的速度进行判断。而在W部分,使用常见文字替代圆点,检测中要求受试者准确指出字体的颜色,而忽略其本身的语义。在C部分中,使用颜色名称矛盾的文字与字体颜色进行替代。
-
采用t(或t′)检验和线性相关分析。
-
依据DMN所涉及的解剖部位选取感兴趣区域(见图 1A~3A)。使用Functool软件对DTI影像数据进行后处理,结果可见对应的感兴趣区纤维束的示踪成像(见图 1B~3B),同时产生ADC图及FA图(见图 1C~3C、1D~3D)。

图 1 DTI示DMN相关脑区的结构
-
TBI后DMN脑区纤维束的受损情况,与对照组相比,TBI组病人个脑区的FA值均降低(P<0.01),TBI组病人gCC的ADC值升高(P<0.01),而Cing、SFOF的ADC值与对照组差异无统计学意义(P>0.05)(见表 1)。
分组 n FA ADC gCC Cing SFOF gCC Cing SFOF 对照组 30 0.56±0.06 0.50±0.04 0.50±0.08 0.68±0.10 0.71±0.10 0.82±0.13 TBI组 45 0.40±0.08 0.34±0.06 0.41±0.10 0.82±0.03 0.74±0.23 0.80±0.37 t — 9.78 15.22* 4.27 7.27* 0.78* 0.34* P — <0.01 <0.01 <0.01 <0.01 >0.05 >0.05 *示t′值 表 1 TBI后FA、ADC的变化(x±s)
-
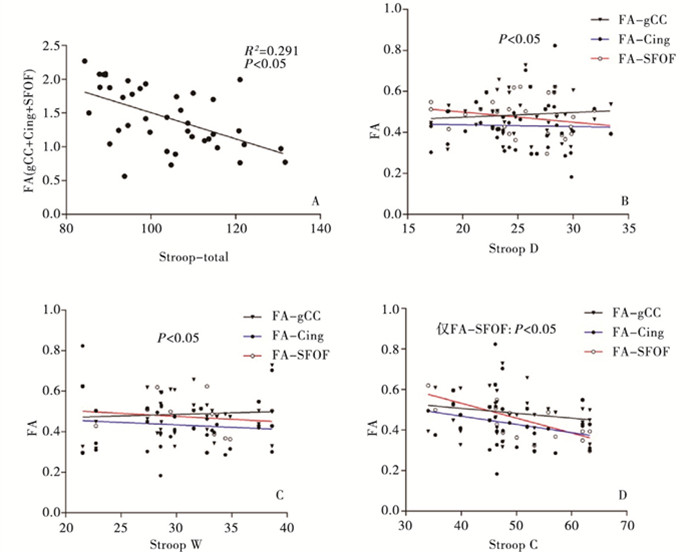
TBI病人的认知功能评估显示,TBI组病人VST各部分耗时数均明显延长(P<0.01)(见表 2)。TBI早期DMN相关脑区(gCC、Cing、SFOF)的影像学特征与注意障碍的关系显示,在TBI病人中,DMN中gCC、Cing、SFOF的FA值之和与VST各部分耗时总和呈负相关关系(P<0.05, R2=0.291)(见图 2A);SFOF的FA值变化与VST中C部分的耗时呈负相关关系(P<0.05, R2=0.396)(见图 2B~D)。
分组 n Stroop D Stroop W Stroop C 对照组 30 18.11±5.14 21.50±2.12 28.46±3.23 TBI组 45 24.01±2.131 26.69±3.12 40.23±7.332 t′ — 5.96 8.58 9.48 P — <0.01 <0.01 >0.05 表 2 TBI后VST评估病人的注意功能(x±s;s)

图 2 TBI病人VST各个部分评分与相应区域FA值的相关性分析
-
TBI是全球性的健康问题,具有病死率高、致残率较高等特点,不仅威胁病人的生命,且影响随后的生活质量[2, 10-12]。除了创伤导致的肢体等神经功能障碍,TBI幸存者多伴有不同程度的心理疾病及认知功能障碍,日常生活受到严重影响[12-16]。其中,注意功能障碍主要表现在处理多个任务时,其信息处理能力及速度降低,并难以保持持续足够的注意力。有学者[17-18, 21]发现注意力控制及障碍形成的结构基础是白质纤维区域连接形成的扩散神经网络。而TBI可通过破坏神经连接,造成神经网络损伤,最终导致工作记忆和注意力缺陷[13-14, 16-17, 19]。在急性期,TBI病人多伴有急性的意识障碍甚至昏迷;即使对于清醒的TBI病人,由于伴有疲劳、烦躁及精神异常等,也难以配合临床医生进行量表评估。现阶段,CT和MRI作为检测和评估TBI严重程度及其局灶性出血、脑挫伤的重要手段。并在基础上,推测病人潜在及长期的认知功能障碍[15-16]。细胞水平的脑损伤在现有的常规CT/MRI数据中无法得到明确的识别。然而,TBI病人却已伴发不同程度的认知功能障碍。因此,如何对TBI病人进行有效的、早期的、客观的认知功能评估仍是当前领域面临的重要问题。
DTI技术是依据水分子移动观察和追踪脑白质纤维束的非侵入性检查方法[6-8]。DTI参数中,反映水分子弥散特征的FA对纤维束完整性评估具有一定价值;ADC可反映脑组织内水分子的整体弥散水平和弥散阻力的情况,两者在TBI病人中具有重要参考价值。既往有学者[13, 20]对TBI后DTI参数值进行分析,并结合认知功能情况,发现DTI的相关数值对认知功能障碍评估具有潜在参考意义。然而,针对于单个纤维束的研究如同“管中窥豹”,影响了认知功能障碍评估的准确性。
大脑的认知功能依赖于大规模分布式脑网络的集成运行,创伤所致认知障碍的结构学基础是神经纤维介导的神经连接中断、缺失[13-14, 21]。在分布式脑网络中,其中,最易评价和识别的是DMN。研究发现DMN参与到注意力和认知行为的调节。随后有学者发现当执行注意性相关的任务时,正常病人存在DMN的激活,而TBI病人存在DMN的激活改变[22]。进一步研究[3]证实,DMN主要涉及的脑结构主要为后扣带回皮层、顶下小叶后部、颞叶内侧结构及腹内侧前额叶皮质。基于上述发现,本研究以DMN为基础,在急性期采用DTI技术对TBI病人进行评估。我们发现与对照组相比TBI病人DMN结构中的FA值明显下降,其变化主要为胼胝体膝部、额枕上束及扣带束的区域。这些区域FA值的急剧下降可能是由于创伤引起的水分子弥散阻力的增加、弥散运动的各向异性降低所致。此外,由于胼胝体位于纵裂底部且血供较为丰富,因而在遭受创伤过程后较易表现出血管性水肿[23]。本研究中,我们也发现胼胝体膝部的ADC值较正常对照明显升高,而其余纤维连接的ADC值变化并无显著差异。因此,TBI急性期FA值降低或ADC值升高为TBI引起DMN结构破坏提供了证据。
注意是大脑控制的心理活动对一定事物的指向和集中,是认知功能的一个重要成分。注意障碍是TBI后认知功能障碍中的一种常见类型,与多个脑区相关[24]。在现有的诊疗过程中,针对TBI病人注意功能障碍的早期识别还存在明显的不足。而基于损伤后单个脑区变化的研究亦不足以对注意障碍进行完整的描述,其主要原因是作为一种高级形式的认知行为,注意依赖于脑网络及其神经连接的综合作用[25]。更为重要的是,现有评估认知功能的量表技术高度依赖病人的配合,存在评估时间长、步骤繁琐等问题。这些缺陷限制了其在TBI后急性期的应用[26-28]。鉴于此,我们通过客观影像学检查发现TBI病人急性期DMN中神经纤维相关的FA值与病人恢复期的注意评分具有一定的相关性。这一结果揭示出基于DMN结构的早期诊断TBI后注意障碍的应用价值。
目前评估注意障碍的方式、工具众多。本研究选用最广泛应用VST量表进行评估。本研究结果显示,TBI病人C部分的耗时数升高最为明显。这可能是由于C部分对病人的注意力和任务复杂度要求最高,使得TBI病人在测试反应的过程中表现出显著的差异。以DMN结构中的特定纤维束进一步分析,我们发现DMN中扣带束的FA值与C部分的耗时呈显著负相关关系,这在一定程度上表明Cing是VST中C部分的主要激活部位。但VST不同部分的耗时数与其余纤维连接的FA值不具有明显的统计学相关性,这可能是由于VST测验任务是借由一个基础更为广泛的系统介导。鉴于这种多因素复杂性,对特定类型注意障碍精确识别,有待于今后更为细分认知测验方式的纳入。
综上,TBI引起纤维连接的中断是损伤后DMN结构破坏的主要因素,而急性期TBI病人脑DMN结构的破坏可作为早期诊断其注意障碍的依据。基于影像学分析DMN结构的变化可作为一项优化指标,这将为注意障碍的客观、早期诊断提供方向,亦为早期干预、预后预测和潜在的疗效评估提供帮助。
基于默认网络结构早期诊断创伤性颅脑损伤后注意障碍的临床研究
Clinical study of the early diagnosis of attention disorder after traumatic brain injury based on default mode network
-
摘要:
目的分析创伤性颅脑损伤(TBI)病人急性期默认网络(DMN)的结构变化,探讨其在早期诊断TBI后注意障碍的应用价值。 方法纳入45例TBI病人作为TBI组,在急性期通过磁共振弥散张量成像技术评估DMN的结构完整性。在恢复期采用注意量表评估病人注意障碍。招募30名健康志愿者作为对照组。分析TBI病人磁共振相关参数,并与对照组进行比较,在此基础上,评估其与认知功能评分的相关性。 结果与对照组相比,TBI病人急性期DMN结构内的各向异性分数(FA)降低(P < 0.01),胼胝体膝部(gCC)的表观弥散系数图(P < 0.01)。在恢复期,TBI病人注意量表评分较对照组均明显延长(P < 0.01)。急性期TBI病人DMN结构的变化与恢复期注意量表的评分显示,TBI病人DMN中扣带束、gCC、额枕上束(SFOF)的FA值之和与Stroop色词量表Victoria版本各部分耗时总和呈负相关关系(P < 0.05,R2=0.291);SFOF的FA值变化与VST中C部分的耗时呈负相关关系(P < 0.05,R2=0.396)。 结论TBI引起纤维连接的中断是损伤后DMN结构破坏的主要因素,DMN结构的破坏可作为早期诊断TBI后注意障碍依据。 Abstract:ObjectiveTo analyze the structural changes of default mode network(DMN) in patients with traumatic brain injury(TBI) in the acute phase, and explore the application value of DMN in the early diagnosis of attention disorder after TBI. MethodsForty-five patients with TBI were set as the TBI group, the structural integrity of DMN was evaluated using diffusion tensor imaging(DTI) during the acute phase, and the attention scale was used to evaluate the patient's attention disorder during convalescence.Thirty healthy volunteers were set as the control group.The MRI-related parameters of TBI patients were analyzed, and compared with the control group.The correlation between the parameters of DTI and cognitive function score was explored. ResultsCompared with the control group, the fractional anisotropy(FA) of brain region decreased(P < 0.01), and the apparent diffusion coefficient(ADC) of genitals of corpus callosum(gCC) increased in the acute phase(P < 0.01).In the convalescence period, the scores of attention scale in TBI patients were significantly longer than those in control group(P < 0.01).The results of the scores of DMN structure changes in the acute phase and scores of convalescence attention scale in the TBI patients showed that the sum of FA value of Cing, gCC and superior occipitofrontal fascicle(SFOF) were negatively correlated with the sumup time of each part of Stroop colour word scale Victoria version(P < 0.05, R2=0.291), and the FA value of SFOF was negatively correlated with the time of part C in VST(P < 0.05, R2=0.396). ConclusionsThe interruption of fiber connection in TBI patients is the key factor of damage of DMN structure.The damage of DMN structure can be used as a useful marker for the early diagnosis of attention disorder. -
Key words:
- traumatic brain injury /
- default mode network /
- attention disorder /
- early diagnosis
-
表 1 TBI后FA、ADC的变化(x±s)
分组 n FA ADC gCC Cing SFOF gCC Cing SFOF 对照组 30 0.56±0.06 0.50±0.04 0.50±0.08 0.68±0.10 0.71±0.10 0.82±0.13 TBI组 45 0.40±0.08 0.34±0.06 0.41±0.10 0.82±0.03 0.74±0.23 0.80±0.37 t — 9.78 15.22* 4.27 7.27* 0.78* 0.34* P — <0.01 <0.01 <0.01 <0.01 >0.05 >0.05 *示t′值  下载: 导出CSV
下载: 导出CSV
表 2 TBI后VST评估病人的注意功能(x±s;s)
分组 n Stroop D Stroop W Stroop C 对照组 30 18.11±5.14 21.50±2.12 28.46±3.23 TBI组 45 24.01±2.131 26.69±3.12 40.23±7.332 t′ — 5.96 8.58 9.48 P — <0.01 <0.01 >0.05
下载: 导出CSV
-
[1] JIANG JY, GAO GY, FENG JF, et al. Traumatic brain injury in China[J]. Lancet Neurol, 2019, 18(3): 286. doi: 10.1016/S1474-4422(18)30469-1 [2] 江基尧. 中国颅脑创伤诊治的未来[J/CD]. 中华神经创伤外科电子杂志, 2019, 5(5): 257. [3] BONNELLE V, LEECH R, KINNUNEN KM, et al. Default mode network connectivity predicts sustained attention deficits after traumatic brain injury[J]. J Neurosci, 2011, 31(38): 13442. doi: 10.1523/JNEUROSCI.1163-11.2011 [4] GREICIUS MD, SUPEKAR K, MENON V, et al. Resting-state functional connectivity reflects structural connectivity in the default mode network[J]. Cereb Cortex, 2009, 19(1): 72. doi: 10.1093/cercor/bhn059 [5] WEISSMAN DH, ROBERTS KC, VISSCHER KM, et al. The neural bases of momentary lapses in attention[J]. Nat Neurosci, 2006, 9(7): 971. doi: 10.1038/nn1727 [6] TAE WS, HAM BJ, PYUN SB, et al. Current clinical applications of diffusion-tensor imaging in neurological disorders[J]. J Clin Neurol, 2018, 14(2): 129. doi: 10.3988/jcn.2018.14.2.129 [7] FILIPPI M, AGOSTA F. Diffusion tensor imaging and functional MRI[J]. Handb Clin Neurol, 2016, 136: 1065. [8] DOUGLAS DB, MULDERMANS JL, WINTERMARK M. Neuroimaging of brain trauma[J]. Curr Opin Neurol, 2018, 31(4): 362. doi: 10.1097/WCO.0000000000000567 [9] 郑锐哲. 基于神经网络早期诊断弥漫性轴索损伤后认知功能障碍的临床研究[D]. 蚌埠: 蚌埠医学院, 2018. [10] 江基尧. 颅脑创伤: 规范与创新[J/CD]. 中华神经创伤外科电子杂志, 2019, 5(2): 65. [11] 马蓉, 高国一, 江基尧. 中国和欧盟颅脑创伤救治中心工作特征比较[J]. 中华创伤杂志, 2019, 35(3): 227. doi: 10.3760/cma.j.issn.1001-8050.2019.03.008 [12] BABIKIAN T, ASARNOW R. Neurocognitive outcomes and recovery after pediatric TBI: meta-analytic review of the literature[J]. Neuropsychology, 2009, 23(3): 283. doi: 10.1037/a0015268 [13] WANG ML, LI WB. Cognitive impairment after traumatic brain injury: The role of MRI and possible pathological basis[J]. J Neurol Sci, 2016, 370: 244. doi: 10.1016/j.jns.2016.09.049 [14] BARMAN A, CHATTERJEE A, BHIDE R. Cognitive impairment and rehabilitation strategies after traumatic brain injury[J]. Indian J Psychol Med, 2016, 38(3): 172. doi: 10.4103/0253-7176.183086 [15] CALVILLO M, IRIMIA A. Neuroimaging and psychometric assessment of mild cognitive impairment after traumatic brain injury[J]. Front Psychol, 2020, 11: 1423. doi: 10.3389/fpsyg.2020.01423 [16] IACCARINO MA, BHATNAGAR S, ZAFONTE R. Rehabilitation after traumatic brain injury[J]. Handb Clin Neurol, 2015, 127: 411. [17] BABIKIAN T, ASARNOW R. Neurocognitive outcomes and recovery after pediatric TBI: meta-analytic review of the literature[J]. Neuropsychology, 2009, 23(3): 283. doi: 10.1037/a0015268 [18] SHARP DJ, SCOTT G, LEECH R. Network dysfunction after traumatic brain injury[J]. Nat Rev Neurol, 2014, 10(3): 156. doi: 10.1038/nrneurol.2014.15 [19] ARENTH PM, RUSSELL KC, SCANLON JM, et al. Corpus callosum integrity and neuropsychological performance after traumatic brain injury: a diffusion tensor imaging study[J]. J Head Trauma Rehabil, 2014, 29(2): E1. [20] 甘剑. 通过DTI观察高压氧对创伤性颅脑损伤病人注意功能障碍的影响[D]. 福州: 福建中医药大学, 2018. [21] WOLF JA, KOCH PF. Disruption of network synchrony and cognitive dysfunction after traumatic brain injury[J]. Front Syst Neurosci, 2016, 10: 43. [22] KIM YH, YOO WK, KO MH, et al. Plasticity of the attentional network after brain injury and cognitive rehabilitation[J]. Neurorehabil Neural Repair, 2009, 23(5): 468. doi: 10.1177/1545968308328728 [23] LI J, LI XY, FENG DF, et al. Quantitative evaluation of microscopic injury with diffusion tensor imaging in a rat model of diffuse axonal injury[J]. Eur J Neurosci, 2011, 33(5): 933. doi: 10.1111/j.1460-9568.2010.07573.x [24] 顾磊, 范家权, 杨光清, 等. 弥漫性轴索损伤后早期磁共振弥散张量成像与恢复期认知功能的相关性研究[J]. 蚌埠医学院学报, 2018, 43(6): 726. [25] CUPAIOLI FA, ZUCCA FA, CAPORALE C, et al. The neurobiology of human aggressive behavior: Neuroimaging, genetic, and neurochemical aspects[J]. Prog Neuropsychopharmacol Biol Psychiatry, 2020, 106: 110059. [26] CARTWRIGHT PE, PERKINS TG, SANTHANAM P, et al. Quantitative analysis tool for clinical functional MRI in mild traumatic brain injury[J]. Undersea Hyperb Med, 2019, 46(3): 245. [27] GOSSELIN N, BOTTARI C, CHEN JK, et al. Electrophysiology and functional MRI in post-acute mild traumatic brain injury[J]. J Neurotrauma, 2011, 28(3): 329. doi: 10.1089/neu.2010.1493 [28] ZHOU Y, LUI YW, ZUO XN, et al. Characterization of thalamo-cortical association using amplitude and connectivity of functional MRI in mild traumatic brain injury[J]. J Magn Reson Imaging, 2014, 39(6): 1558. doi: 10.1002/jmri.24310 -

 点击查看大图
点击查看大图

图(2)表(2)
计量
- 文章访问数: 3431
- HTML全文浏览量: 1920
- PDF下载量: 9
- 被引次数: 0
