





-
传统开放性甲状腺手术创伤明显,影响术后美观,病人的接受度不高[1]。腔镜甲状腺手术可降低创伤,利于恢复,已被广泛应用[2-3],并且已经相对成熟,但不少学者对腔镜甲状腺手术给机体带来的应激创伤方面存在质疑。此外,临床中缺少甲状腺手术对于机体的应激创伤因子相关方面的研究,没有充分的理论依据。白细胞(WBC)、血糖(Glu)、C反应蛋白(CRP)以及促肾上腺皮质激素(ACTH)作为机体应激反应的相关因子,可以一定程度上反映机体的创伤程度。本研究通过动态检测以上创伤因子的水平变化,探讨不同甲状腺手术方式对于病人身体应激的影响。
-
选取2018年6月至2020年10月于我院行经单侧甲状腺肿瘤手术的病人90例,分为3组:腋窝组32例、胸乳组28例、常规组30例。腋窝组男4例,女28例,25~55岁;胸乳组男3例,女25例,25~51岁;常规组男4例,女26例,23~52岁。3组均为单侧腺叶病变,均无手术禁忌,手术方式由病人自行选择。3组病人性别、年龄等一般资料均具有可比性。病人及其家人均知情同意。
-
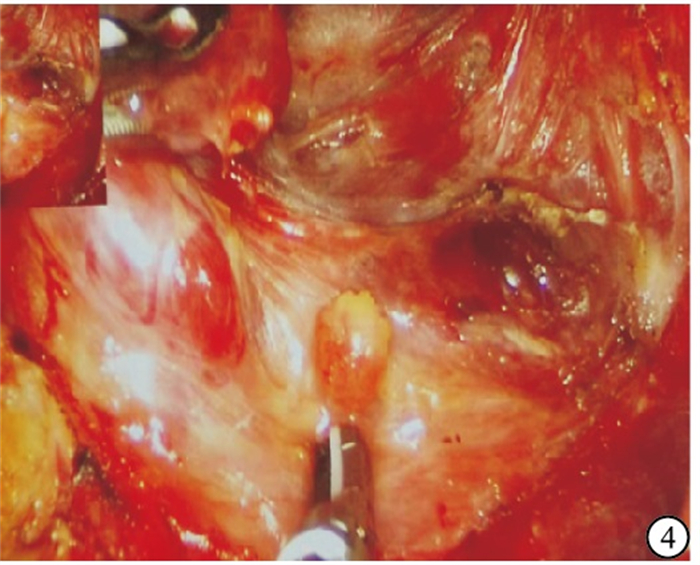
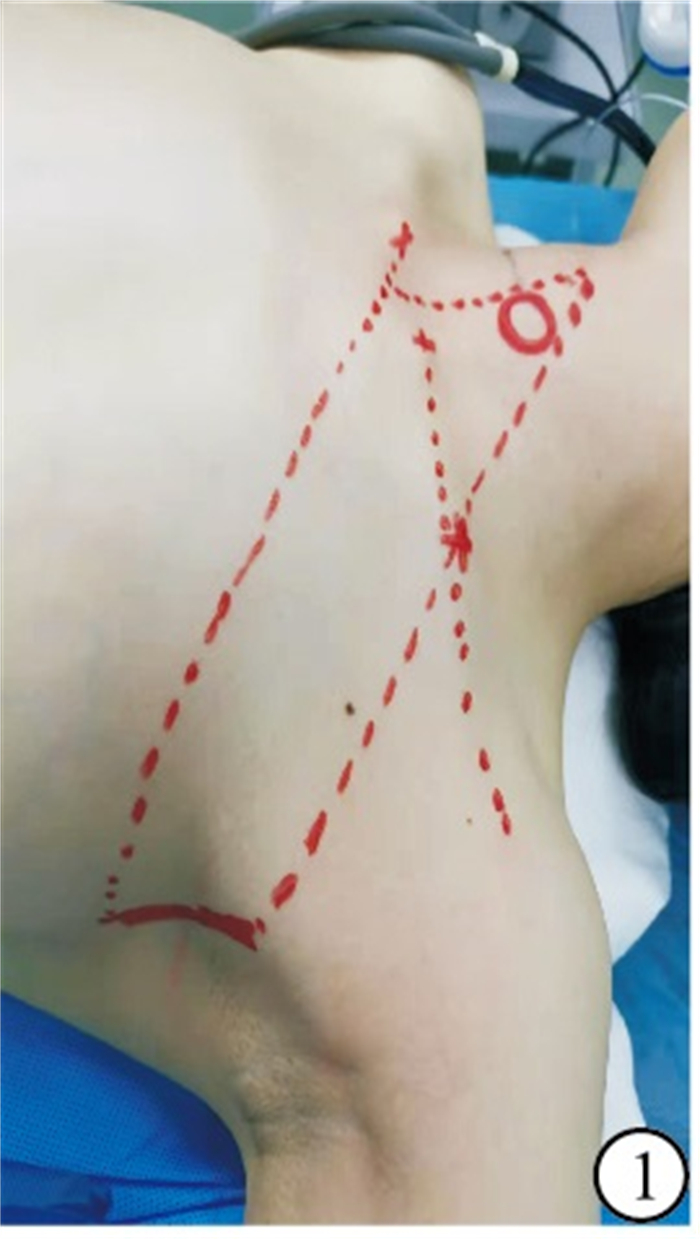
腋窝入路腔镜甲状腺手术。(1)仰卧位,用标记笔画出胸骨上切迹中点、患侧锁骨中点与胸大肌外侧缘的垂线,延伸至腋中线;自锁骨中点至胸大肌外侧缘的垂线交点开始,尽量沿腋下皮纹在腋前线及腋中线向内下作3~5 cm切口(见图 1)。(2)建腔,切开腋下“内上-外下”斜形切口,沿胸大肌筋膜表面向病灶方向建立腔道(见图 2);钝性锐性结合逐层打开胸锁乳突肌下段间隙(见图 3),裸游离并裸化肩胛舌骨肌,并于其后方显露颈内静脉,沿颈内静脉向上向下充分游离,最大限度拉开肌肉空间,以利于拉钩进入带状肌下方;继续游离甲状腺区域周围组织,上、下、内侧分别至甲状腺上极、锁骨头以及峡部。(3)左手钳固定并向下牵拉甲状腺上极,注意牵拉力度适当,避免用力过度影响超声刀凝血效果;超声刀断上极应做到完全包裹血管,逐步自上而下“脱帽”,做到原位保留甲状旁腺(见图 4)。(4)中央区淋巴结清扫,腔镜的放大作用可以帮助顺利并且非常清晰地找到喉返神经,沿着喉返神经由下而上清除淋巴脂肪组织,在清除的过程中应在腔镜的辅助下时刻关注甲状旁腺的位置,随后将切除标本送常规病理检查。冲洗术腔,彻底止血。

图 1 腋窝入路体表标记操作范围

图 2 腋窝入路建腔
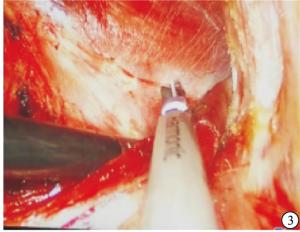
图 3 腋窝入路胸锁乳突肌间隙
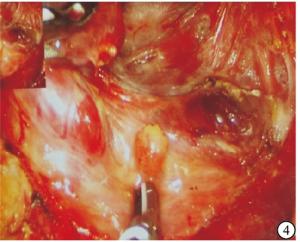
图 4 腔镜下甲状旁腺的保留
-
胸乳入路腔镜甲状腺手术。(1)平卧位,体表标记,两侧内上乳晕切口及内乳边缘近胸骨切口,分别长0.8~1.0、0.8~1.0、1.0~1.2 cm的切口(见图 5)。(2)建腔,切开颈白线,其余步骤同上。

图 5 胸乳人路体表标记
-
常规开放甲状腺手术。病人取仰卧位、颈部横切口、游离皮瓣、断颈白线(见图 6)等,其余同上。

图 6 开放甲状腺手术颈白线切开
-
检测术前及术后1、3 d早晨6点病人空腹WBC、Glu、CRP、ACTH水平。指尖Glu由我科使用血糖仪检测,WBC、CRP由我院检验科检测,ACTH由核医学科实验室检测。
-
采用χ2检验、方差分析和q检验。
-
3组术前WBC、CRP、Glu、ACTH水平及术后3 d Glu水平差异均无统计学意义(P>0.05);3组术后1、3 d WBC、CRP、Glu、ACTH水平均高于术前(P < 0.05);3组术后1 d WBC、CRP、Glu、ACTH水平均高于术后3 d(P < 0.05);术后1、3 d,常规组、腋窝组、胸乳组WBC、CRP、ACTH水平逐渐降低(P < 0.01)(见表 1)。
分组 n 术前 术后1 d 术后3 d F P MS组内 WBC 常规组 30 5.39±1.48 11.01±2.63▲ 8.59±1.71▲■ 59.45 < 0.011 4.010 腋窝组 32 5.59±1.38 9.71±1.83*▲ 7.59±1.38*▲■ 56.93 < 0.011 2.386 胸乳组 28 5.71±1.79 8.18±1.42*#▲ 6.51±1.39*#▲■ 21.32 < 0.011 2.384 F — 0.32 14.07 13.91 — — — P — >0.05 < 0.011 < 0.011 — — — MS组内 — 2.403 4.125 2.253 — — — CRP 常规组 30 2.81±0.69 24.87±6.77▲ 18.13±6.79▲■ 124.46 < 0.011 30.804 腋窝组 32 2.61±0.76 18.91±5.81*▲ 13.75±5.19*▲■ 108.74 < 0.011 20.423 胸乳组 28 2.69±0.68 15.01±4.67*#▲ 9.53±4.11*#▲■ 81.72 < 0.011 13.054 F — 0.61 21.10 17.75 — — — P — >0.05 < 0.011 < 0.011 — — — MS组内 — 0.508 34.074 30.208 — — — Glu 常规组 30 4.69±0.61 5.99±0.55*▲ 5.11±0.49▲■ 43.31 < 0.011 0.305 腋窝组 32 4.89±0.54 5.51±0.49*▲ 5.07±0.48■ 12.82 < 0.011 0.254 胸乳组 28 4.79±0.62 5.59±0.63*▲ 5.10±0.47▲■ 13.64 < 0.01 0.334 F — 0.89 6.48 0.06 — — — P — >0.05 < 0.01 >0.05 — — — MS组内 — 0.347 0.310 0.231 — — — ACTH 常规组 30 24.01±8.96 68.01±16.11▲ 45.45±16.57▲■ 70.92 < 0.01 204.793 腋窝组 32 23.12±8.87 57.12±16.87*▲ 35.87±13.87*▲■ 50.97 < 0.01 185.217 胸乳组 28 22.23±7.29 45.13±15.97*#▲ 26.88±9.39*#▲■ 31.05 < 0.01 132.119 F — 0.32 14.20 13.34 — — — P — >0.05 < 0.01 < 0.01 — — — MS组内 — 71.288 267.069 187.434 — — — q检验:与常规组比较*P < 0.05;与腋窝组比较#P < 0.05;与术前比较▲P < 0.05;与术后1 d比较■P < 0.05 表 1 3组WBC、CRP、Glu和ACTH水平比较(x±s,n;×105/L)
-
手术作为疾病的治疗方案在临床中的地位举足轻重,治疗效果显而易见,但手术给机体带来的创伤同样也是不可忽视的。过度的应激反应会引发机体内分泌、代谢等改变[4-6]。当机体在受到手术等应激创伤时,会激活下丘脑-垂体-肾上腺轴,引起肝脏急性期反应,促使体内ACTH、Glu、CRP、WBC等水平的改变。因此,机体在应对手术创伤产生的细胞因子及内分泌激素水平的变化可以作为监测并反映机体受到创伤轻重程度的指标。腔镜甲状腺手术的独特优势使其在治疗甲状腺肿瘤疾病本身、保障病人生命安全健康的同时,满足了病人的美容要求,减少病人的心里压力和精神负担。
在应对外界应激创伤时,肝脏产生的急性应激反应可诱发外周血中WBC水平的提高,并且提升的程度与创伤的严重程度呈正相关关系,因此,WBC的水平变化可作为衡量个体应激反应程度的指标。WBC作为机体创伤严重程度的检测指标之一,技术上方便易行,经济上成本较低,易于普及和推广应用。本研究中,3组病人均未出现切口、肺部、泌尿系及身体其他部位感染。排除以上因素,发现3组病人围手术期WBC水平发生了动态改变,术前处于正常水平,术后升高,尤其是术后第1天,检测值达到最高状态;另外,观察结果提示三种甲状腺手术方式对病人血液中WBC值影响程度相比亦有差异,常规组影响最大,腋窝组次之,胸乳组最小。证实了手术作为一种创伤,是诱导病人血液中WBC水平升高的因素,也验证了WBC作为衡量个体应激反应的高敏感性,间接反映2组腔镜甲状腺手术带给病人的应激创伤并不比传统开放式手术大;相反,胸乳入路相较于其他两种方式对机体的创伤更小,而传统开放式甲状腺手术对病人身体的创伤可能最大。
手术可引起机体CRP水平变化。3组术后1、3 d CRP水平均高于术前。其理论基础是个体受到手术创伤的打击,诱发机体发生肝脏急性期反应,使之产生较大量的CRP。另外,手术创伤可抑制分泌胰岛素及胰岛素受体[7]。因此,在排除感染等其他因素的情况下,CRP水平一定程度上可以直观地反映机体受到创伤的严重程度,即CRP作为机体应激指标之一,机体受到的创伤越重,CRP水平升高越明显。本研究结果显示,3组病人术后CRP水平均不同程度的升高,其中,胸乳组给机体带来的创伤应激对升高病人外周血中CRP水平影响最小,常规组则影响最大,腋窝组介于两者之间。笔者认为,该结果可以在一定程度上直观地体现出3种手术对病人身体的创伤程度。此外,创伤对胰岛素分泌的抑制同样在一定程度上改变着病人围手术期的Glu水平。3组病人术后均出现了Glu水平升高,验证了Glu作为应激因子的敏感性。本研究中,3种手术方式对病人Glu水平均有影响,在短时间内,常规组影响最大,腋窝组次之,胸乳组最小;但随着时间的推移,通过机体的自身调节会使体内升高的Glu很快恢复至正常。
手术开始后较短时间内就可检测出外周血中ACTH水平的升高[8]。本研究结果发现,围手术期3组病人的ACTH的检测值前后发生了明显的改变,手术带来的创伤刺激了病人外周血中ACTH值的升高,同前面3个实验指标相似,ACTH水平的高低同样反应着病人因手术所造成对身体创伤的严重程度。从3种手术方式对机体ACTH值的影响来看, 常规组影响最大, 胸乳组最小。这样的结果可能是基于腔镜的放大优势、术中出血量少、超声刀的稳定性、术中牵拉的程度较轻以及切口较小等因素。而胸乳组在对机体应激创伤影响上要小于腋窝组,原因可能是胸乳组是最接近于开放手术的方式的腔镜手术,自然间隙寻找容易,术中对周围正常组织损伤较小。
腔镜甲状腺手术美容效果好[9-12],疼痛轻[13],但手术时间较长[14-15]。较好的腔镜基础是开展腔镜甲状腺手术的重要前提之一[16];同时,术者对器械的要求越来越高,金功圣等[17]将免充气腔镜甲状腺器械不断改进,更新换代,功能上已上升至可行免充气侧颈淋巴结清扫。
本研究发现,腔镜甲状腺手术比传统手术更能减缓人体所受刺激,因此在一定程度上提高了病人的生活质量。目前,随着医学科学的发展及人们对健康需求的不断提升,对腔镜甲状腺手术进行更深入研究已势在必行。本研究还存在一些不足之处:病例数相对较少,原因是腔镜甲状腺手术在本病区起步较晚,在筛选病例的过程中对于手术指征的把握相对严格,以致在较长时间内收集较少病例;观察指标需进一步完善。
不同甲状腺手术方式对机体应激的影响
Effects of different thyroid surgery methods on body stress
-
摘要:
目的探讨胸乳入路、腋窝入路腔镜甲状腺手术以及常规开放甲状腺手术对机体应激创伤的影响。 方法选取行甲状腺手术的病人90例,根据自愿选择手术方式分为胸乳组28例、腋窝组32例和常规组30例。比较3组病人术前、术后1、3 d的白细胞(WBC)、血糖(Glu)、C反应蛋白(CRP)和促肾上腺皮质激素(ACTH)水平。 结果3组术前WBC、CRP、Glu、ACTH水平及术后3 d Glu水平差异均无统计学意义(P>0.05);3组术后1、3 d WBC、CRP、Glu、ACTH水平均高于术前(P < 0.05);3组术后1 d WBC、CRP、Glu、ACTH水平均高于术后3 d(P < 0.05);术后1、3 d,常规组、腋窝组、胸乳组WBC、CRP、ACTH水平逐渐降低(P < 0.01)。 结论腔镜甲状腺手术对机体应激的影响低于开放甲状腺手术。 Abstract:ObjectiveTo investigate the effects of endoscopic thyroid surgery via thoraco mammary approach approach, axillary approach and conventional open thyroid surgery on stress trauma. MethodsNinety patients undergoing thyroid surgery were divided into in the thoraco mammary group(n=28), axillary group(n=32) and conventional group(n=30).The levels of white blood cell(WBC), blood glucose(Glu), C reactive protein(CRP) and adreno-cortico-tropic-hormone(ACTH) in the three groups were compared before operation, 1 day and 3 days after operation. ResultsThere was no significant difference in the levels of WBC, CRP, Glu, ACTH before operation, and Glu at 3 days after operation among the three groups(P>0.05).The levels of WBC, CRP, Glu and ACTH in the three groups at 1 day and 3 days after operation were higher than those before operation(P < 0.05).The levels of WBC, CRP, Glu and ACTH in the three groups at 1 day after operation were higher than those at 3 days after operation(P < 0.05).At 1 day and 3 days after operation, the levels of WBC, CRP and ACTH gradually decreased in the conventional group, axillary group and thoraco mammary group(P < 0.01). ConclusionsThe endoscopic thyroid surgery has lower effects on stress than open thyroid surgery. -
Key words:
- thyroid neoplasms /
- thyroid surgery /
- endoscopy /
- stress
-
表 1 3组WBC、CRP、Glu和ACTH水平比较(x±s,n;×105/L)
分组 n 术前 术后1 d 术后3 d F P MS组内 WBC 常规组 30 5.39±1.48 11.01±2.63▲ 8.59±1.71▲■ 59.45 < 0.011 4.010 腋窝组 32 5.59±1.38 9.71±1.83*▲ 7.59±1.38*▲■ 56.93 < 0.011 2.386 胸乳组 28 5.71±1.79 8.18±1.42*#▲ 6.51±1.39*#▲■ 21.32 < 0.011 2.384 F — 0.32 14.07 13.91 — — — P — >0.05 < 0.011 < 0.011 — — — MS组内 — 2.403 4.125 2.253 — — — CRP 常规组 30 2.81±0.69 24.87±6.77▲ 18.13±6.79▲■ 124.46 < 0.011 30.804 腋窝组 32 2.61±0.76 18.91±5.81*▲ 13.75±5.19*▲■ 108.74 < 0.011 20.423 胸乳组 28 2.69±0.68 15.01±4.67*#▲ 9.53±4.11*#▲■ 81.72 < 0.011 13.054 F — 0.61 21.10 17.75 — — — P — >0.05 < 0.011 < 0.011 — — — MS组内 — 0.508 34.074 30.208 — — — Glu 常规组 30 4.69±0.61 5.99±0.55*▲ 5.11±0.49▲■ 43.31 < 0.011 0.305 腋窝组 32 4.89±0.54 5.51±0.49*▲ 5.07±0.48■ 12.82 < 0.011 0.254 胸乳组 28 4.79±0.62 5.59±0.63*▲ 5.10±0.47▲■ 13.64 < 0.01 0.334 F — 0.89 6.48 0.06 — — — P — >0.05 < 0.01 >0.05 — — — MS组内 — 0.347 0.310 0.231 — — — ACTH 常规组 30 24.01±8.96 68.01±16.11▲ 45.45±16.57▲■ 70.92 < 0.01 204.793 腋窝组 32 23.12±8.87 57.12±16.87*▲ 35.87±13.87*▲■ 50.97 < 0.01 185.217 胸乳组 28 22.23±7.29 45.13±15.97*#▲ 26.88±9.39*#▲■ 31.05 < 0.01 132.119 F — 0.32 14.20 13.34 — — — P — >0.05 < 0.01 < 0.01 — — — MS组内 — 71.288 267.069 187.434 — — — q检验:与常规组比较*P < 0.05;与腋窝组比较#P < 0.05;与术前比较▲P < 0.05;与术后1 d比较■P < 0.05  下载: 导出CSV
下载: 导出CSV
-
[1] MAKINO T. In properly selected patients with differentiated thyroid cancer, antithyroglobulin antibodies decline after thyroidectomy and their sole presence should not be an indication for radioiodine ablation[J]. Arch Endocrin Metab, 2019, 63(3): 130. [2] HAO J, JINRUI F, KUN L, et al. A propensity score matching study between ultrasound-guided percutaneous microwave ablation and conventional thyroidectomy for benign thyroid nodules treatment[J]. Int J Hyperther, 2018, 35(1): 125. [3] WANG T, WU Y, XIE Q, et al. Safety of central compartment neck dissection for transoral endoscopic thyroid surgery in papillary thyroid carcinoma[J]. Jpn J Clin Oncol, 2020, 50(4): 387. doi: 10.1093/jjco/hyz195 [4] DESBOROUGH JP. The stress response to trauma and surgery[J]. Br J Anaesth, 2000, 85(1): 109. doi: 10.1093/bja/85.1.109 [5] ESME H, SOLAK O, YURUMEZ Y, et al. The factors affecting the morbidity and mortality in chest trauma[J]. Ulus Travma Derg, 2006, 12(4): 305. [6] WU J, SHENG L, MA Y, et al. The analysis of risk factors of impacting mortality rate in severe multiple trauma patients with posttraumatic acute respiratory distress syndrome[J]. Am J Emerg Med, 2008, 26(4): 419. doi: 10.1016/j.ajem.2007.06.032 [7] YAMAUCHI T, KAMON J, WAKI H, et al. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity[J]. Nat Med, 2001, 7(8): 941. doi: 10.1038/90984 [8] DESBOROUGH JP. The stress response to trauma and surgery[J]. Brit J Anaesth, 2000, 85(1): 109. doi: 10.1093/bja/85.1.109 [9] ANUWONG A, KETWONG K, JITPRATOOM P, et al. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach[J]. JAMA Surg, 2018, 153(1): 21. doi: 10.1001/jamasurg.2017.3366 [10] 彭文, 彭小伟, 李赞, 等. 经口入路腔镜手术在较大甲状腺良性肿瘤中的应用[J]. 临床耳鼻咽喉头颈外科杂志, 2018, 32(13): 972. [11] YANG SC, AHN JH, KIM JH, et al. Comparison of the vessel sealer extend with harmonic ACE in robotic bilateral axillary-breast approach thyroid surgery[J]. Gland Surg, 2020, 9(2): 164. doi: 10.21037/gs.2020.01.18 [12] YULIAN ED, KURNIA A, KARTINI D, et al. Endoscopic thyroidectomy via axillary-breast-shoulder approach: early experience of 42 cases[J]. Surg Oncol, 2020, 34: 318. doi: 10.1016/j.suronc.2020.05.007 [13] 孙思雨, 张晨嵩, 谢波, 等. 经腋窝入路免充气全腔镜甲状腺癌根治术和开放甲状腺癌根治术疗效对比[J]. 蚌埠医学院学报, 2021, 46(2): 173. [14] 徐加杰, 张李卓, 张启弘, 等. 无充气经腋窝腔镜甲状腺手术的临床应用[J]. 中华耳鼻咽喉头颈外科杂志, 2020, 55(10): 913. doi: 10.3760/cma.j.cn115330-20200225-00126 [15] 李景铧, 张帆, 张毅, 等. 全腔镜与开放手术治疗cT1N0甲状腺乳头状癌的临床对比研究[J]. 第三军医大学学报. 2019, 41(15): 1461. [16] 王平, 燕海潮. 腔镜甲状腺手术常见问题及其对策[J]. 腹腔镜外科杂志, 2018, 23(4): 11. [17] 金功圣, 张浩, 陈沿松, 等. 免充气腔镜器械在经全乳晕入路腔镜甲状腺手术中的应用[J]. 蚌埠医学院学报, 2021, 46(4): 455. -

 点击查看大图
点击查看大图
图(6)表(1)
计量
- 文章访问数: 2152
- HTML全文浏览量: 1150
- PDF下载量: 4
- 被引次数: 0
