

-
非器质性失眠症是国际疾病分类第10版(ICD-10)使用的术语,指一组以情绪为原发病因或主要诱因的一种失眠症亚型,据相关研究表明,全球33%~50%的成人主诉每年有数夜失眠,长期的失眠对人类的注意力控制、警觉性、脑力负荷状态等带来显著的负面影响[1],更是心血管疾病、广泛性焦虑、抑郁、人体免疫力降低等疾病的危险因素[2-3],严重降低生活质量、工作效率,损害社会功能,甚至导致恶性意外事故的发生,是一个亟需解决的公共卫生健康问题。与其他疾病的诊断不同,非器质性失眠症的临床诊断目前是严格基于主观报告,缺乏客观便捷的评估方法[4]。而脑电波的发现和记录使得睡眠成为一种可量化的行为,可以准确判断和分析人类睡眠状态[5-6],暂时临床上公认多导睡眠监测(polysomnography,PSG)是监测睡眠的金标准[4]。但是由于主观报告的不准确性、PSG的复杂不便性,急需探求一种更为便捷客观的评估手段来丰富对非器质性失眠症的诊断。本研究采集非器质性失眠症和健康人群任务态脑电,分析事件相关电位P300成分的振幅和潜伏期差异性,并通过溯源分析方法探讨二者脑区溯源的特征,为临床提供一种更为客观准确的评估方法和日后睡眠障碍精准医学奠定基础。
-
非器质性失眠组:招募蚌埠医学院2022年1-6月的非器质性失眠症在校大学生10例,其中男5例,女5例,年龄18~30岁。入组标准:(1)符合ICD-10[7];(2)无其他睡眠障碍,如睡眠异常、睡眠过多、睡眠相关运动障碍或其他精神障碍;(3)爱丁堡利手量表测量的右手性;(4)裸视或矫正视力正常;(5)性别不限,年龄≥18岁且愿意参加本研究,并签署知情同意书。排除标准:(1)孕期、哺乳期或月经期;(2)器质性疾病或继发于抑郁或广泛性焦虑的严重精神疾病所致的失眠;(3)神经系统或其他躯体疾病史,如呼吸、心脏、肾脏、肝脏和内分泌疾病;(4)1个月内任何可能影响睡眠或脑功能的药物;(5)成瘾障碍;(6)脑电数据质量差。健康对照组:与非器质性失眠症组同期招募的健康在校大学生10名,其中男3名,女7名,年龄18~30岁。入组标准:(1)良好的睡眠质量和良好的睡眠开始和/或维持,匹兹堡睡眠质量指数(Pittsburgh sleep quality index,PSQI)低于5分;(2)本研究前至少2个星期未服用任何兴奋剂、药物、香烟、酒精或咖啡;(3)爱丁堡利手量表测量的右手性;(4)裸视或矫正视力正常;(5)性别不限,年龄≥18岁且愿意参加本研究,并签署知情同意书。排除标准同非器质性失眠症组。本研究方案经蚌埠医学院伦理委员会批准审核(伦科批字[2022]第336号)。所有受试者自愿参加本研究,并签署知情同意书。2组受试者性别、年龄均有可比性。
-
所有受试者均需要进行神经心理学评估,从主观上了解受试者睡眠情况和心理健康程度,包括PSQI、汉密尔顿焦虑量表(Hamilton anxiety scale,HAMA)、汉密尔顿抑郁量表(Hamilton depression scale,HAMD)。PSQI包括主观睡眠质量、睡眠潜伏期、睡眠时间、习惯睡眠效率、睡眠紊乱累加问题、催眠药物、日间功能障碍七个成份(18个条目),每个成份按0~3等级计分,累计各成份得分为PSQI总分,总分为0~21分,得分越高表示睡眠质量越差;HAMA包括14个成份,每个成份按0~4等级计分,总分56分,得分越高表示焦虑程度越高;HAMD包括17个成份,每个成份按照0~2、0~4等级计分,总分58分,得分越高表示抑郁程度越严重。
-
采用E-prime 2.0软件编写N-back任务,任务难度(N值)为0~2。在本任务中,电脑显示屏中央随机呈现1个介于0~9的数字,要求被试判断当前呈现的数字与n个之前呈现的数字是否相同(如:N=0时,即0-back任务中,被试需判断当前数字是否等于“3”),并使用键盘“F”键(代表是),和键盘“J”键(代表否)作出反应,所有刺激大小均相等,刺激为白色,背景为黑色。当前数字呈现的时间为1 000 ms,随即呈现“+”注视点,时间为1 000 ms,按照固定刺激间隔呈现下一个数字,一个难度系数的测试总计为75次。受试者测试各难度水平的N-back任务的数字顺序是以伪随机的概率交叉出现,每一难度水平的N-back任务时间约为3 min,任务间隙受试者可决定是否短暂休息,以避免精神疲劳。
本实验在隔音、弱光、室温20~25 ℃的实验室中进行。首先要求受试者确保头发清洁,参照国际10/20系统安置法佩戴脑电极帽。本研究脑电数据通过EGI脑电设备(USA)和国际10-20系统扩展的128导HydroCel高密度网状电极帽采集记录。所有电极点阻抗均 < 50 kΩ,采样率为1 000 Hz。在线参考为Cz,离线分析转为平均参考。在正式采集脑电数据之前,要求受试者自然放松与舒适座椅上。在采集过程中,要求受试者保持平静,面部肌肉放松,避免晃动头部、眼球漂移、咀嚼、吞咽、睡觉等动作的发生,仅按主试者指令进行操作。
-
任务态脑电数据于Net Station中Waveform Tools进行ERP分析。对采集的脑电数据依次予以滤波、分段、伪迹处理、坏通道替换、平均参考、基线校正、转换参考等。其中带通滤波参数为0.1~30 Hz;根据预先设定好的mark将事件分段,截取刺激前100 ms到刺激后1 000 ms,且将标准刺激和目标刺激分开,其中以刺激前100 ms作为基线校正;伪迹处理主要去除坏电极、眨眼和眼动,每640 ms时间窗中,最大值和最小值差值>640 μV视为坏通道,>140 μV视为眨眼,>55 μV的视为眼动;采用全脑平均参考;根据临床上试验上已有的ERP成分分析,选择提取Fz、Cz、Pz的P3的振幅和潜伏期,P3成分的时间窗为刺激呈现后250~500 ms[8]。
-
溯源分析数据在Net Station中的GeoSource工具栏中进行。建立以AC-PC中点为原点的三维立体坐标系,获得大脑冠状面图像上顶内沟的三维立体坐标值,以标准化低分辨率脑电磁断层扫描方法进行溯源定位,对2组受试者溯源特征属性进行分析对比。主要提取激活区域强度、三维坐标点、Brodmann脑区等。
-
采用t检验、秩和检验和Fisher′s确切概率法。
-
非器质性失眠症组PSQI总分及其各个组成部分评分、HAMA评分、HAMD评分均高于健康对照组(P < 0.05~P < 0.01)(见表 1)。2组在0-back、1-back任务中的正确率、反应时间差异均无统计学意义(P>0.05),2组在2-back任务中的正确率、反应时间差异均有统计学意义(P < 0.05)(见表 2)。
分组 n PSQI总分 主观睡眠质量 睡眠潜伏期 睡眠时间 习惯睡眠效率 睡眠紊乱累加问题 催眠药物 日间功能障碍 HAMA评分 HAMD评分 非器质性失眠症组 10 11.90±1.52 2.20±0.42 2.70±0.48 1.70±0.68 1.50±0.85 1.70±0.68 0 2.10±0.88 13.20±8.47 18.30±12.34 健康对照组 10 4.10±0.74 1.00±0.47 0.90±0.74 0.20±0.42 0.30±0.48 1.00±0.00 0 0.70±0.68 4.40±3.57 3.50±2.72 t — 14.57 600 6.45 5.96 3.88 3.28 — 4.01 3.03 3.7 P — < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 — < 0.01 < 0.01 < 0.05 表 1 2组神经心理学评估结果比较(x±s;分)
N-back 非器质性失眠症组
(n=10)健康对照组
(n=10)t P 0-back 正确率/% 96.00±4.11 97.40±3.27 1.54 >0.05 反应时间/ms 605.82±49.01 659.21±91.42 1.63 >0.05 1-back 正确率/% 90.20±5.45 93.40±4.43 3.40 >0.05 反应时间/ms 722.09±103.29 722.57±81.50 0.01 >0.05 2-back 正确率/% 75.40±7.55 81.20±3.80 4.95 < 0.05 反应时间/ms 970.64±154.28 842.34±98.79 2.22 < 0.05 表 2 2组行为学数据结果比较(x±s)
-
非器质性失眠症组在0-back任务中Fz点、1-back任务中Fz点的P300振幅均低于健康对照组(P < 0.05和P < 0.01)(见表 3)。非器质性失眠症组在2-back任务中Fz、Cz、Pz点的P300潜伏期均长于健康对照组(P < 0.05)(见表 4)。
相关因素 非器质性失眠症组
(n=10)健康对照组
(n=10)t P 0-back Fz 2.90±1.63 5.60±2.93 2.55 < 0.05 Cz 3.53(2.11,4.88) 3.46(2.83,3.83) -0.08△ >0.05 Pz 4.23(2.45,12.80) 7.48(1.96,11.56) -0.38△ >0.05 1-back Fz 2.82±2.12 6.72±3.74 2.87 < 0.01 Cz 2.57(1.94,3.54) 2.72(0.04,3.94) -0.45△ >0.05 Pz 4.69(3.34,6.94) 5.53(4.01,9.08) -1.06△ >0.05 2-back Fz 3.91(2.53,5.47) 4.50(3.55,10.37) -0.98△ >0.05 Cz 2.37±0.98 2.66±1.83 0.43 >0.05 Pz 4.19(1.09,6.89) 1.93(0.99,5.88) -0.53△ >0.05 △示uc值 表 3 2组P300振幅比较(x±s;μV)
相关因素 非器质性失眠症组
(n=10)健康对照组
(n=10)t P 0-back Fz 271.50(253.75,325.00) 291.50(277.75,346.75) -1.44△ >0.05 Cz 293.00(259.75,436.25) 396.50(283.00,444.25) -0.91△ >0.05 Pz 464.10±29.96 431.70±47.32 1.83 >0.05 1-back Fz 315.40±70.23 307.40±56.01 0.28 >0.05 Cz 346.70±78.86 371.70±86.35 0.68 >0.05 Pz 455.30±48.02 473.50±22.32 1.09 >0.05 2-back Fz 380.20±94.99 289.70±37.80 2.80 < 0.05 Cz 404.50(360.00,446.75) 264.50(250.00,332.50) -2.44△ < 0.05 Pz 408.70±84.25 334.40±47.14 2.43 < 0.05 △示uc值 表 4 2组P300潜伏期比较(x±s;ms)
-
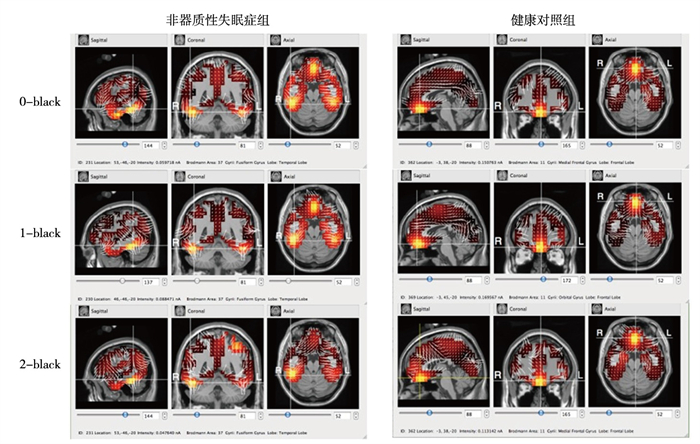
任务态溯源脑区主要集中在额叶部分,非器质性失眠症组激活区域较为分散,且在0-back和2-back中激活区域电流强度明显低于健康对照组(P < 0.01)(见图 1、表 5)。

图 1 2组在N-back任务中P300溯源分析结果
分组 n 0-back 1-back 2-back 非器质性失眠症组 10 0.07(0.06,0.10) 0.08(0.07,0.22) 0.08±0.04 健康对照组 10 0.16(0.11,0.24) 0.14(0.08,0.19) 0.29±0.20 uc — -2.80 -0.68 3.15△ P — < 0.01 >0.05 < 0.01 △示t值 表 5 2组溯源激活区域电流强度比较[M(P25,P75);nA]
-
非器质性失眠症是以情绪为原发病因或主要诱因的一种失眠症亚型,其表现主要有入睡困难,或夜间经常醒来,难以维持睡眠,或睡眠治疗差,常常对日间功能带来显著的负面影响。
工作记忆是人类认知的核心,是对信息进行短暂储存和操控的系统,在执行控制、记忆方面起着关键的作用,且相关研究表明,失眠会引起大脑功能的改变,影响病人工作记忆的能力,是当前国际上认知心理学和认知神经科学领域中最活跃的研究热点之一,可以在一定程度上反映大脑处理、控制的能力[9],而ERP中的P300成分恰好代表高级认知水平的信息处理,如注意力、控制力、理解和判断等,其振幅反映执行任务过程中大脑资源的分配,潜伏期则反映了大脑对刺激进行评估、决策的耗时[10]。DRUMMOND等[11]通过MRI观察在工作记忆期间原发性失眠病人的大脑区域激活情况,并提出失眠症受试者显示出与任务相关的工作记忆区域的激活减少。由于神经影像学技术受到它们所测定的皮质关系的相关性的限制[12],尚不能准确把握外界刺激时同步诱发的大脑皮层神经元活动,目前对于区域间的功能连接还在探索中,因此任务态EEG提供了克服这一局限的有效方法,直接评估大脑执行任务时,信号在时间和空间上向解剖学和功能连接的大脑区域的传播。本研究结果显示,随着工作记忆任务负荷的增加,所有受试者的行为学数据中正确率下降,反应时间增加,ERP成分中P300振幅增加、潜伏期延长,但相较于健康对照组,非器质性失眠症组改变幅度略小;组间比较结果中也显示,非器质性失眠症组在0-back和1-back任务中Fz点的波幅、2-back任务中Fz、Cz、Pz的潜伏期均显示有统计学差异。由此可以证明长时间睡眠不佳在一定程度上会对大脑执行任务上产生显著的负面影响,若失眠状况持续未得到改善,可能会带来更加严重的影响。
在全球关注“脑计划”的时代大背景下,人脑是一个大规模的网络,其功能依赖于空间分布区域之间的动态连接作用。脑电图记录的是大脑皮层的神经元集群突触后电位的电势,关键特征是具有高时间分辨率,脑电溯源定位即为脑电的逆向分析,根据头皮各个电极的时域信号,反演估计脑内神经活动源的位置、方向和强度信息,从而实现事件相关电位的源定位和某些频段脑电功率的源定位[13-14]。在临床应用中,对大脑活动源的无创定位可用于诊断与大脑相关的病理、生理、心理和功能异常,非常适合任务中大脑活动的评估[15]。通过溯源分析,可以准确的掌握执行任务时在大脑皮层的传播特征,估算失眠症病人脑功能异常的信号源定位,并且结合大脑Brodmann分区,本研究对受试者进行任务态P300溯源分析发现健康对照组在执行工作记忆任务中,激活脑区主要分布于额叶,多为Brodmann分区中的11,且激活区域的电流较大,在0-back和2-back任务中中明显高于非器质性失眠症组。而非器质性失眠症组在执行任务时激活区域较为分散,这可能与执行工作记忆任务时投入的精力、注意力有密切关系。
目前国内外对失眠症的热点研究以采用fMRI、PET等影像学技术为多数[16-17],虽然fMRI、PET的具有高空间分辨率,却暂不能在时间轴线纵断面上探讨失眠症病人脑网络节点、脑区关联性、可塑性的科学机制,本研究在任务态背景下,以毫秒级别的高时间分辨率上分析ERP特征和脑功能区之间的差异,补充时间层面研究的空缺,为以后从时间和空间双重层面探讨非器质性失眠症的脑机制、神经电生理研究及多模态影像学融合,完成动态特性分析,进一步预防和治疗失眠症病人伴随的执行功能障碍、认知障碍等提供有力的指导依据,实现精准评估、精准治疗、精准康复,具有前瞻性。
综上所述,非器质性失眠症ERP特征及溯源脑区方面存在一定的差异,有望成为非器质性失眠症者,甚至其他睡眠障碍的评估的客观手段,目前需继续扩大样本,增加结果的可信度。
基于P300的非器质性失眠症ERP特征及溯源分析
ERP characteristics and source analysis of non-organic insomnia based on P300
-
摘要:
目的探讨非器质性失眠症在事件相关电位下的P300特征和溯源分析。 方法将受试者分为健康对照组和非器质性失眠症组, 各10例, 采用EGI高密度脑电设备记录受试者任务态脑电及行为学数据, 其中任务态脑电选择数字N-back任务。通过Net Station软件分析事件相关电位, 提取Fz、Cz、Pz电极点的P300潜伏期、振幅以及行为学数据, 并在GeoSource工具栏中进行溯源定位。比较2组溯源特征属性。 结果非器质性失眠症组匹兹堡睡眠质量指数总分及其各个组成部分评分、汉密尔顿焦虑量表评分、汉密尔顿抑郁量表评分均高于健康对照组(P < 0.05~P < 0.01)。2组在0-back、1-back任务中的正确率、反应时间差异均无统计学意义(P>0.05), 2组在2-back任务中的正确率、反应时间差异均有统计学意义(P < 0.05)。非器质性失眠症组在0-back任务中Fz点、1-back任务中Fz点的P300振幅均低于健康对照组(P < 0.05和P < 0.01)。非器质性失眠症组在2-back任务中Fz、Cz、Pz点的P300潜伏期均长于健康对照组(P < 0.05)。任务态溯源脑区主要集中在额叶部分, 非器质性失眠症组激活区域较为分散, 且在0-back和2-back中激活区域电流强度明显低于健康对照组(P < 0.01)。 结论非器质性失眠症受试者大脑工作记忆略有受损, 分散了大脑认知资源, 降低了大脑执行等高级认知能力, 因此基于P300的事件相关电位特征和溯源分析结果可在一定条件下对其进行客观评估, 并且其便捷性值得以后在临床上推广。 Abstract:ObjectiveTo explore the P300 characteristics and source analysis of non-organic insomnia at event-related potential. MethodsThe subjects were divided into healthy control group (n=10) and non-organic insomnia group (n=10).The task state electroencephalogram and behavioral data of the subjects were recorded with EGI high-density electroencephalogram equipment, and the task state electroencephalogram was selected for the digital N-back task.The event-related potential was analyzed through Net Station software to extract P300 latency, amplitude and behavioral data from the Fz, Cz and Pz electrode points, and to to locate the source in the GeoSource toolbar.The source characteristics was compared between the two groups. ResultsThe total score of Pittsburgh sleep quality index and its components, Hamilton anxiety scale score, Hamilton depression scale score in the non-organic insomnia group were higher than those in the healthy control group (P < 0.05 to P < 0.01).There was no significant difference in the accuracy and reaction time between the two groups in the 0-back and 1-back tasks (P>0.05), and there was significant difference in the accuracy and reaction time between the two groups in the 2-back task (P < 0.05).The P300 amplitude of Fz point in 0-back task and Fz point in 1-back task in non-organic insomnia group was lower than that in healthy control group (P < 0.05 and P < 0.01).The P300 latency of Fz, Cz, Pz points in the 2-back task in the non-organic insomnia group was longer than that in the healthy control group (P < 0.05).The source brain regions of task state were mainly concentrated in the frontal lobe.The active regions in the non-organic insomnia group were scattered, and the current intensity of the active regions in 0-back and 2-back was significantly lower than that in the healthy control group (P < 0.01). ConclusionsSubjects with non-organic insomnia have slightly impaired working memory of brain, which distracts the cognitive resources of brain and reduces higher cognitive abilities such as brain execution.Therefore, the characteristics of event-related potential based on P300 and source analysis can be objectively assessed under certain conditions, and the convenience of which warrants future clinical promotion. -
Key words:
- non-organic insomnia /
- event-related potential /
- P300 /
- electroencephalogram source
-
表 1 2组神经心理学评估结果比较(x±s;分)
分组 n PSQI总分 主观睡眠质量 睡眠潜伏期 睡眠时间 习惯睡眠效率 睡眠紊乱累加问题 催眠药物 日间功能障碍 HAMA评分 HAMD评分 非器质性失眠症组 10 11.90±1.52 2.20±0.42 2.70±0.48 1.70±0.68 1.50±0.85 1.70±0.68 0 2.10±0.88 13.20±8.47 18.30±12.34 健康对照组 10 4.10±0.74 1.00±0.47 0.90±0.74 0.20±0.42 0.30±0.48 1.00±0.00 0 0.70±0.68 4.40±3.57 3.50±2.72 t — 14.57 600 6.45 5.96 3.88 3.28 — 4.01 3.03 3.7 P — < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 < 0.01 — < 0.01 < 0.01 < 0.05  下载: 导出CSV
下载: 导出CSV
表 2 2组行为学数据结果比较(x±s)
N-back 非器质性失眠症组
(n=10)健康对照组
(n=10)t P 0-back 正确率/% 96.00±4.11 97.40±3.27 1.54 >0.05 反应时间/ms 605.82±49.01 659.21±91.42 1.63 >0.05 1-back 正确率/% 90.20±5.45 93.40±4.43 3.40 >0.05 反应时间/ms 722.09±103.29 722.57±81.50 0.01 >0.05 2-back 正确率/% 75.40±7.55 81.20±3.80 4.95 < 0.05 反应时间/ms 970.64±154.28 842.34±98.79 2.22 < 0.05
下载: 导出CSV
表 3 2组P300振幅比较(x±s;μV)
相关因素 非器质性失眠症组
(n=10)健康对照组
(n=10)t P 0-back Fz 2.90±1.63 5.60±2.93 2.55 < 0.05 Cz 3.53(2.11,4.88) 3.46(2.83,3.83) -0.08△ >0.05 Pz 4.23(2.45,12.80) 7.48(1.96,11.56) -0.38△ >0.05 1-back Fz 2.82±2.12 6.72±3.74 2.87 < 0.01 Cz 2.57(1.94,3.54) 2.72(0.04,3.94) -0.45△ >0.05 Pz 4.69(3.34,6.94) 5.53(4.01,9.08) -1.06△ >0.05 2-back Fz 3.91(2.53,5.47) 4.50(3.55,10.37) -0.98△ >0.05 Cz 2.37±0.98 2.66±1.83 0.43 >0.05 Pz 4.19(1.09,6.89) 1.93(0.99,5.88) -0.53△ >0.05 △示uc值
下载: 导出CSV
表 4 2组P300潜伏期比较(x±s;ms)
相关因素 非器质性失眠症组
(n=10)健康对照组
(n=10)t P 0-back Fz 271.50(253.75,325.00) 291.50(277.75,346.75) -1.44△ >0.05 Cz 293.00(259.75,436.25) 396.50(283.00,444.25) -0.91△ >0.05 Pz 464.10±29.96 431.70±47.32 1.83 >0.05 1-back Fz 315.40±70.23 307.40±56.01 0.28 >0.05 Cz 346.70±78.86 371.70±86.35 0.68 >0.05 Pz 455.30±48.02 473.50±22.32 1.09 >0.05 2-back Fz 380.20±94.99 289.70±37.80 2.80 < 0.05 Cz 404.50(360.00,446.75) 264.50(250.00,332.50) -2.44△ < 0.05 Pz 408.70±84.25 334.40±47.14 2.43 < 0.05 △示uc值
下载: 导出CSV
表 5 2组溯源激活区域电流强度比较[M(P25,P75);nA]
分组 n 0-back 1-back 2-back 非器质性失眠症组 10 0.07(0.06,0.10) 0.08(0.07,0.22) 0.08±0.04 健康对照组 10 0.16(0.11,0.24) 0.14(0.08,0.19) 0.29±0.20 uc — -2.80 -0.68 3.15△ P — < 0.01 >0.05 < 0.01 △示t值
下载: 导出CSV
-
[1] 黄杨森, 邵帅, 程耀萍, 等. N-back任务诱导梯度脑力负荷状态对失匹配负波振幅的影响[J]. 人类工效学, 2019, 25(1): 11. [2] MAHMOOD A, RAY M, DOBALIAN A, et al. Insomnia symptoms and incident heart failure: a population-based cohort study[J]. Eur Heart J, 2021, 42(40): 4169. doi: 10.1093/eurheartj/ehab500 [3] 刘灿, 汪立. 妊娠期糖尿病孕妇睡眠质量与感知压力、心理韧性的相关性研究[J]. 蚌埠医学院学报, 2022, 47(8): 1134. doi: 10.13898/j.cnki.issn.1000-2200.2022.08.033 [4] RIEMANN D, BAGLIONI C, BASSETTI C, et al. European guideline for the diagnosis and treatment of insomnia[J]. J Sleep Res, 2017, 26(6): 675. doi: 10.1111/jsr.12594 [5] GRIMALDI D, REID KJ, PAPALAMBROS NA, et al. Autonomic dysregulation and sleep homeostasis in insomnia[J]. Sleep, 2021, 44(6): 1. [6] LONG S, DING R, WANG J, et al. Sleep quality and electroencephalogram delta power[J]. Front Neurosci, 2021, 15: 803507. doi: 10.3389/fnins.2021.803507 [7] UYSAL S. ICD-10-CM diagnosis coding for neuropsychological assessment[J]. Arch Clin Neuropsychol, 2019, 34(5): 721. doi: 10.1093/arclin/acy084 [8] GONGORA M, NICOLICHE E, MAGALHAES J, et al. Event-related potential (P300): the effects of levetiracetam in cognitive performance[J]. Neurol Sci, 2021, 42(6): 2309. doi: 10.1007/s10072-020-04786-8 [9] ROSE NS, LAROCQUE JJ, RIGGALL AC, et al. Reactivation of latent working memories with transcranial magnetic stimulation[J]. Science, 2016, 354(6316): 1136. doi: 10.1126/science.aah7011 [10] GUTIERREZ-ZAMORA VELASCO G, FERNANDEZ T, SILVA-PEREYRA J, et al. Higher cognitive reserve is associated with better working memory performance and working-memory-related P300 modulation[J]. Brain Sci, 2021, 11(3): 1. [11] DRUMMOND SP, WALKER M, ALMKLOVl E, et al. Neural correlates of working memory performance in primary insomnia[J]. Sleep, 2013, 36(9): 1307. doi: 10.5665/sleep.2952 [12] HAWCO C, VOINESKOS AN, STEEVES JKE, et al. Spread of activity following TMS is related to intrinsic resting connectivity to the salience network: a concurrent TMS-fMRI study[J]. Cortex, 2018, 108: 160. doi: 10.1016/j.cortex.2018.07.010 [13] HABIB MA, IBRAHIM F, MOHKTAR MS, et al. Recursive independent component analysis (ICA)-decomposition of ictal EEG to select the best ictal component for EEG source imaging[J]. Clin Neurophysiol, 2020, 131(3): 642. doi: 10.1016/j.clinph.2019.11.058 [14] CONDE V, TOMASEVIC L, AKOPIAN I, et al. The non-transcranial TMS-evoked potential is an inherent source of ambiguity in TMS-EEG studies[J]. Neuroimage, 2019, 185: 300. doi: 10.1016/j.neuroimage.2018.10.052 [15] MAHJOORY K, NIKULIN VV, BOTREL L, et al. Consistency of EEG source localization and connectivity estimates[J]. Neuroimage, 2017, 152: 590. doi: 10.1016/j.neuroimage.2017.02.076 [16] KIM YB, KIM N, LEE JJ, et al. Brain reactivity using fMRI to insomnia stimuli in insomnia patients with discrepancy between subjective and objective sleep[J]. Sci Rep, 2021, 11(1): 1592. doi: 10.1038/s41598-021-81219-2 [17] LEE MH, KIM N, YOO J, et al. Multitask fMRI and machine learning approach improve prediction of differential brain activity pattern in patients with insomnia disorder[J]. Sci Rep, 2021, 11(1): 9402. doi: 10.1038/s41598-021-88845-w -

 点击查看大图
点击查看大图
图(1)表(5)
计量
- 文章访问数: 1761
- HTML全文浏览量: 739
- PDF下载量: 26
- 被引次数: 0
