

-
肺癌是各种癌症相关死亡的首要原因[1-2]。其中小细胞肺癌(small cell lung cancer, SCLC)恶性程度高,占比10%~15%。该类肿瘤生长快速,早期容易出现远处转移,具有高度侵袭性和致命性,这些特点导致大多数SCLC病人在确诊时已处于疾病晚期阶段,预后极差[3]。近年来,PD-L1抑制剂如Atezolizumab、Durvalumab让广泛期小细胞肺癌(ES-SCLC)的治疗有了一些突破[4-5],但由于该类制剂在中国上市较国外晚,且上市后价格昂贵,导致单纯化疗在一段时间内将仍然是ES-SCLC的主流方案。一线化疗是该类疾病的基石,但有效的疗效预测方法和预后判断生物标志物的缺乏在一定程度上限制了病人的获益。近年来,免疫炎症指标淋巴细胞-单核细胞比值(lymphocyte to monocyte ratio, LMR)协助判断包括SCLC在内的多种恶性肿瘤的疗效和预后的作用被多项研究[6-10]所证实。其中GO等[9]发现,诊断时的LMR可预测在接受一线化疗或放化疗的SCLC病人的疗效和预后,但该研究没有对局限期和广泛期SCLC进行区分。QI等[11]在研究基线LMR对使用免疫联合化疗治疗ES-SCLC病人预后预测价值时发现,LMR并不是其独立预后因素。可见,LMR在ES-SCLC病人中的临床价值值得进一步探索。本研究选择接受一线化疗的ES-SCLC病人,探讨LMR对病人一线化疗疗效及生存的预测价值。
-
回顾性收集2019年1月至2022年1月在我院肿瘤内科治疗的50例ES-SCLC病人临床资料。纳入标准:经组织学或细胞学确诊为SCLC;经影像学确诊为广泛期;可测量病灶≥1个;接受一线标准化疗方案治疗≥2个周期;临床资料完整且可被追溯。排除标准:合并其他肿瘤及亚型;合并使用其他抗肿瘤治疗手段;既往接受过针对晚期阶段的系统治疗。
-
纳入病人均接受“铂类联合依托泊苷”或“铂类联合伊立替康”的双药方案治疗。具体参考美国国立综合癌症网络、中国临床肿瘤学会等国内外SCLC诊疗指南或规范。收集病人性别、年龄、吸烟史、ECOG评分、病理资料、浆膜腔积液情况、原发灶情况、远处转移情况、疗效评价情况和进展时间等临床资料。通过医院复查或电话随访等方式获取病人病情进展时间和死亡时间,随访截止日期为2022年3月。记录病人一线化疗前外周血淋巴细胞、单核细胞计数,并计算LMR:LMR=外周血淋巴细胞计数(109/L)/外周血单核细胞计数(109/L)。根据受试者工作特征(receiver operating characteristic, ROC)曲线确定LMR最佳截断值,取最大约登指数时所对应的指标值,将病人分为高、低LMR 2组,比较2组ES-SCLC病人一线化疗疗效和预后的差异。
-
近期疗效参照实体肿瘤疗效评价标准(RECIST)1.1版进行,包括:完全缓解(complete response, CR)、部分缓解(partial response, PR)、疾病稳定(stable disease, SD)和疾病进展(progressive disease, PD)。疾病控制率(disease control rate, DCR)=(CR+PR+SD)/(CR+PR+SD+PD),客观有效率(objective response rate, ORR)=(CR+PR)/(CR+PR+SD+PD)。远期疗效观察无进展生存时间(progression-free survival,PFS)和总生存时间(overall survival,OS)。PFS:病人从开始一线治疗至出现疾病进展或死亡的时间,OS:病人从开始一线治疗至因任何原因导致死亡的时间。
-
采用t检验、χ2检验;应用Kaplan-Meier法绘制2组生存曲线,采用log-rank检验比较;使用Cox回归分析筛选预后因素。均为双侧检测,检测水准为α=0.05。
-
纳入ES-SCLC病人共50例,年龄45~88岁,男45例(90%)。基线LMR与病人是否患有低蛋白血症和骨转移有关(P < 0.05);而年龄、性别、吸烟状况、ECOG评分、有无肺部炎症、有无浆膜腔积液、有无脏器、脑以及肝转移均与基线LMR无关(P>0.05)(见表 1)。
变量 n LMR t P 性别 男
女45
53.04±1.15
2.87±1.710.30 >0.05 年龄/岁 ≤60
>6017
333.08±1.21
2.99±1.210.23 >0.05 吸烟 否
是34
163.21±1.19
2.63±1.161.61 >0.05 ECOG评分/分 0~1
232
183.19±1.16
2.72±1.241.37 >0.05 白蛋白/(g/L) < 35.0
≥35.07
432.12±0.77
3.17±1.202.24 < 0.05 肺部炎症 否
是16
342.76±1.07
3.15±1.251.06 >0.05 浆膜腔积液 否
是24
263.33±1.10
2.74±1.241.79 >0.05 脏器转移 否
是15
353.26±1.17
2.92±1.210.91 >0.05 脑转移 否
是39
112.96±1.25
3.26±1.030.73 >0.05 肝转移 否
是28
223.15±1.14
2.86±1.280.84 >0.05 骨转移 否
是28
223.32±1.08
2.64±1.262.05 < 0.05 表 1 ES-SCLC病人基线血清LMR与临床特征的关系(x±s)
-
50例ES-SCLC病人一线化疗后,CR 0例,PR 25例,SD 18例,PD 7例。ORR为50.0%,DCR为86.0%。LMR最佳截断值为3.08,高LMR组22例,化疗疗效评价为CR或PR的病人15例,PD或SD为7例;低LMR组28例,化疗疗效评价为CR或PR的病人10例,PD或SD为18例。分析发现,基线LMR越高,一线化疗疗效越好(χ2=5.20,P < 0.05)(见表 2)。
分组 n PD+SD PR+CR χ2 P 低LMR组 28 18 10 高LMR组 22 7 15 5.20 < 0.05 合计 50 25 25 表 2 ES-SCLC病人基线血清LMR与一线化疗疗效的关系(n)
-
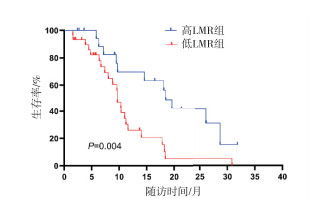
50例病人中位PFS为7.4个月。LMR最佳截断值为3.16,其中高LMR组20例,低LMR组30例,中位PFS分别为9.0个月与5.8个月。生存结果分析提示,PFS在高、低LMR组间差异有统计学意义(χ2=4.50, P < 0.05)(见图 1)。单因素Cox回归分析表明,有无脏器转移和基线LMR与PFS相关(P < 0.05)(见表 3)。将有无脏器转移和基线LMR纳入多因素Cox回归分析,结果显示,有无脏器转移和基线LMR均是ES-SCLC病人PFS的独立预测因素(P < 0.05)(见表 4)。

图 1 ES-SCLC病人血清LMR与PFS的生存曲线分析
变量 B SE Waldχ2 P HR(95%CI) 性别 -0.842 0.488 2.98 >0.05 0.431(0.165~1.122) 年龄 -0.214 0.361 0.35 >0.05 0.808(0.398~1.638) 吸烟 0.006 0.342 0.00 >0.05 1.006(0.515~1.966) ECOG评分 0.069 0.338 0.04 >0.05 1.071(0.552~2.077) 白蛋白 -0.846 0.453 3.48 >0.05 0.429(0.177~1.044) 肺部炎症 0.048 0.393 0.02 >0.05 1.049(0.485~2.268) 浆膜腔积液 -0.105 0.323 0.11 >0.05 0.900(0.478~1.697) 脏器转移 0.897 0.412 4.74 < 0.05 2.451(1.093~5.496) 脑转移 0.056 0.402 0.02 >0.05 1.057(0.481~2.327) 肝转移 0.411 0.331 1.54 >0.05 1.508(0.788~2.886) 骨转移 -0.608 0.339 3.21 >0.05 0.545(0.280~1.058) LMR -0.722 0.348 4.30 < 0.05 0.486(0.246~0.961) 表 3 ES-SCLC病人PFS的单因素Cox回归分析
变量 B SE Waldχ2 P HR(95%CI) 脏器转移 0.867 0.408 4.52 < 0.05 2.381(1.070~5.297) LMR -0.698 0.347 4.05 < 0.05 0.498(0.252~0.982) 表 4 ES-SCLC病人PFS的多因素Cox回归分析
-
50例病人中位OS为11.0个月。LMR最佳截断值为3.16,其中高LMR组20例,低LMR组30例,中位OS分别为18.5个月和9.7个月。生存结果分析提示,OS在高、低LMR组间差异有统计学意义(χ2=8.47, P < 0.01)(见图 2)。单因素Cox分析显示,性别、有无脏器转移和基线LMR与OS相关(P < 0.05~P < 0.01)(见表 5)。将性别、有无脏器转移和基线LMR纳入多因素Cox回归分析,结果显示,性别、有无脏器转移和基线LMR均是ES-SCLC病人OS的独立预测因素(P < 0.05~P < 0.01)(见表 6)。

图 2 ES-SCLC病人血清LMR与OS的生存曲线分析
变量 B SE Waldχ2 P HR(95%CI) 性别 -1.54 0.524 8.63 < 0.01 0.214(0.077~0.599) 年龄 -0.127 0.395 0.10 >0.05 0.881(0.406~1.910) 吸烟 -0.069 0.355 0.04 >0.05 0.933(0.466~1.871) ECOG评分 0.096 0.354 0.07 >0.05 1.101(0.550~2.205) 白蛋白 -0.381 0.464 0.67 >0.05 0.683(0.275~1.696) 肺部炎症 -0.122 0.439 0.08 >0.05 0.885(0.374~2.092) 浆膜腔积液 -0.364 0.353 1.06 >0.05 0.695(0.348~1.388) 脏器转移 0.869 0.441 3.88 < 0.05 2.384(1.004~5.663) 脑转移 0.126 0.429 0.09 >0.05 1.135(0.490~2.628) 肝转移 0.495 0.37 1.79 >0.05 1.641(0.794~3.388) 骨转移 0.033 0.353 0.01 >0.05 1.034(0.518~2.063) LMR -1.084 0.387 7.86 < 0.01 0.338(0.158~0.722) 表 5 ES-SCLC病人OS的单因素Cox回归分析
变量 B SE Waldχ2 P HR(95%CI) 性别 -1.253 0.522 5.77 < 0.05 0.286(0.103~0.794) 脏器转移 1.006 0.453 4.94 < 0.05 2.735(1.126~6.644) LMR -1.130 0.406 7.74 < 0.01 0.323(0.146~0.716) 表 6 ES-SCLC病人OS的多因素Cox回归分析
-
本研究纳入的50例病人,一线化疗的近期疗效评价指标ORR为50.0%、DCR为86.0%,远期疗效评价指标中位PFS为7.4个月、中位OS为11.0个月。国际研究[5]中卡铂联合依托泊苷化疗组的中位PFS 4.3个月、中位OS 10.3个月。CHENG等[12]研究中,顺铂联合依托泊苷作为ES-SCLC病人一线治疗方案的ORR为53.9%、DCR为85.5%,中位PFS为5.3个月、中位OS为9.7个月。其中,本研究PFS相较于临床试验长,考虑是病人未能接受和临床试验一样严密的医学观察,复查不规律或者影像学评估滞后所致。本研究其余疗效评价指标与临床试验高度一致,可见,本中心研究数据具有一定的代表性。
近年来,肿瘤与免疫、炎症反应的关系被广泛研究。肿瘤细胞在免疫逃逸的同时,可以通过全身炎症反应创造有利的微环境,来促进其自身生长、侵袭和转移[13]。淋巴细胞包括CD8+细胞毒性T细胞(CD8+ cytotoxic T cells, CTL)和CD4+辅助性T细胞(CD4+ helper T cells, Th),是免疫系统的主要成分。CTL可通过组织相容复合体Ⅰ类分子杀伤肿瘤细胞,Th主要通过激活CTL、NK细胞,及产生肿瘤坏死因子等发挥免疫作用[14]。因此,淋巴细胞减少将导致机体抗肿瘤免疫应答能力减弱,使肿瘤易于进展和扩散,进而影响病人的治疗效果和转归。外周血淋巴细胞计数的减少与包括ES-SCLC在内的多种恶性肿瘤病人较短的OS相关[15-17],因此,本研究推断淋巴细胞计数可有效反映宿主的免疫功能,从而影响预后。单核细胞可参与病原体的清除和炎症反应,与此同时,其在粒细胞-巨噬细胞集落刺激因子和白细胞介素(IL)-4的作用下可刺激T淋巴细胞活化[18],因此单核细胞也是免疫细胞的重要组成部分。单核细胞趋化到肿瘤组织后,可分化成肿瘤相关巨噬细胞(tumor-associated macrophages, TAMs)。TAMs是肿瘤组织中炎症浸润的重要部分,可促进许多生长因子等物质的产生,进而促进肿瘤侵袭和迁移[19-20]。另外,TAMs和肿瘤细胞可通过产生IL-10来削弱CTL的抗肿瘤反应[21],从而帮助肿瘤细胞发生免疫逃逸。因此,肿瘤相关的炎症反应可抑制机体免疫力。我们推测,结合这两个参数获得的LMR可对机体的免疫应答能力和肿瘤负荷水平进行有效评估。
本研究结果显示,由基线血清淋巴细胞和单核细胞计数计算所得的LMR值是ES-SCLC独立预后指标,LMR越低,预后越差。淋巴细胞计数低、单核细胞计数高提示宿主免疫应答能力较差和肿瘤负荷较重,往往反映肿瘤病人的预后不佳。这与之前LMR对多种恶性肿瘤预后影响的研究[8-10]结果相一致,共同支持较低的LMR与ES-SCLC病人较短的PFS和OS相关这一研究发现。关于PFS、OS的Cox回归分析结果表明,有无脏器转移是PFS、OS的独立预测指标,性别和OS相关。MINAMI等[22]发现,有无脏器转移是ES-SCLC病人的独立预后因素,因为肿瘤负荷会影响病人预后;而性别与OS不相关。但许文娟等[23]发现,性别是SCLC病人的独立预后指标,可能与基因易感性、激素水平等对生存状况产生的影响相关。因此,性别与ES-SCLC病人OS的相关性尚待进一步明确。
另外本研究还发现,基线LMR可预测ES-SCLC的一线化疗疗效,体现在LMR越低,化疗疗效越差。这与既往在多种肿瘤上探索LMR的疗效预测价值的研究[6-8]发现一致。TAMs可通过增加肿瘤基质密度、诱导肿瘤细胞发生上皮间充质转化等过程,影响化疗药物进入肿瘤细胞,同时增强肿瘤细胞自身抗凋亡能力,从而参与肿瘤的化疗耐药[24]。而且,由单核巨噬细胞产生的IL-6也被发现可通过分泌抗凋亡蛋白增加肺癌对化疗药物的耐药性[25]。这些研究均支持LMR有作为恶性肿瘤化疗疗效预测标志物的潜在价值。
本研究在对LMR与ES-SCLC临床变量关系分析时发现,低蛋白血症、骨转移病人LMR更低。在应答肿瘤过程中,单核巨噬细胞通过分泌肿瘤坏死因子α,进而抑制白蛋白的合成;另外其释放的炎症因子损伤内皮细胞,也可以导致毛细血管通透性增加,血清白蛋白漏出,因此LMR指标一定程度上可以间接反映血清白蛋白含量, 这一点也在其他恶性肿瘤的研究[26]中得到证实。肺癌骨转移大多是溶骨型病变,扩散到骨髓中的肿瘤细胞可分泌多种炎症因子,这些细胞因子通过激活RANKL通路产生成熟的破骨细胞,引起骨吸收[27]。淋巴细胞可直接或间接杀伤肿瘤细胞,因此骨转移病人外周血淋巴细胞计数可能相对较低,同时该类病人因炎症因子释放影响单核细胞计数,导致其LMR倾向于更低。
综上所述,LMR是一种计算简便、易于获得的免疫炎症指标,有作为预测ES-SCLC病人一线化疗疗效和预后生物标志物的潜在价值,未来检测基线LMR对于该类病人的疾病管理具有重要意义。但本研究结果基于小样本的单中心回顾性数据,在本研究结论推广前需更大样本量的多中心前瞻性研究对其进行验证。
LMR对广泛期小细胞肺癌一线化疗疗效和预后的预测价值
Value of LMR in predicting the efficacy of first-line chemotherapy and prognosis for extensive-stage small cell lung cancer
-
摘要:
目的探讨免疫炎症指标淋巴细胞-单核细胞比值(LMR)预测广泛期小细胞肺癌(ES-SCLC)病人一线化疗疗效和预后的价值。 方法回顾性收集符合本研究纳入标准的ES-SCLC病人临床资料, 计算LMR, 应用ROC曲线选择最佳截断值, 分为高LMR组和低LMR组, 分析2组一线化疗疗效、无进展生存时间(PFS)和总生存时间(OS)的差异。 结果共纳入50名ES-SCLC病人, 临床特征分析提示, 基线LMR与病人是否患有低蛋白血症和骨转移有关(P < 0.05)。高、低LMR组客观缓解率分别为68.2%和35.7%, 疾病控制率分别为90.9%和82.1%;基线LMR越高, 化疗疗效越好(P < 0.05)。高低2组中位PFS分别为9.0个月与5.8个月, 中位OS分别为18.5个月与9.7个月。Cox回归分析提示, 基线LMR是ES-SCLC病人一线治疗PFS和OS的独立预测因素(P < 0.05~P < 0.01)。 结论LMR有望成为评估ES-SCLC病人一线化疗应答和预后的新指标, 低LMR病人的疗效和预后较差。 -
关键词:
- 小细胞肺癌 /
- 广泛期 /
- 淋巴细胞-单核细胞比值 /
- 一线化疗 /
- 预后
Abstract:ObjectiveTo investigate the value of immune-inflammation index lymphocyte to monocyte ratio (LMR) in predicting the efficacy of first-line chemotherapy and also the prognosis in patients with extensive-stage small cell lung cancer (ES-SCLC). MethodsThe clinical data of ES-SCLC patients eligible for the inclusion criteria of this study were retrospectively collected.The LMR value were calculated, and the optimal cut-off value was selected based on receiver operating characteristic (ROC) curve.The patients were then divided into high- and low-LMR groups.The efficacy and progression-free survival (PFS) of first-line chemotherapy, and overall survival (OS) of patients in high- and low-LMR groups were finally analyzed. ResultsA total of 50 patients with ES-SCLC were included and divided into high- and low-LMR groups.Analyses of clinical characteristics showed that baseline LMR was associated with hypoproteinemia and bone metastasis(P < 0.05).The objective response rates were 68.2% and 35.7%, and the disease control rates were 90.9% and 82.1%, in patients in high- and low-LMR groups, respectively.Better efficacy of first-line chemotherapy can be achieved in patients with higher baseline LMR (P < 0.05).The median PFS in the high- and low-LMR groups were 9.0 and 5.8 months, and the median OS were 18.5 and 9.7 months, respectively.The Cox regression analyses results showed that LMR is an independent predictor of both PFS and OS in ES-SCLC patients treated with first-line chemotherapy(P < 0.05 to P < 0.01). ConclusionsLMR has the potential to sever as a new predictor of the treatment response of first-line chemotherapy and prognosis for patients with ES-SCLC, and the population with low LMR value tend to demonstrate poor efficacy and prognosis. -
表 1 ES-SCLC病人基线血清LMR与临床特征的关系(x±s)
变量 n LMR t P 性别 男
女45
53.04±1.15
2.87±1.710.30 >0.05 年龄/岁 ≤60
>6017
333.08±1.21
2.99±1.210.23 >0.05 吸烟 否
是34
163.21±1.19
2.63±1.161.61 >0.05 ECOG评分/分 0~1
232
183.19±1.16
2.72±1.241.37 >0.05 白蛋白/(g/L) < 35.0
≥35.07
432.12±0.77
3.17±1.202.24 < 0.05 肺部炎症 否
是16
342.76±1.07
3.15±1.251.06 >0.05 浆膜腔积液 否
是24
263.33±1.10
2.74±1.241.79 >0.05 脏器转移 否
是15
353.26±1.17
2.92±1.210.91 >0.05 脑转移 否
是39
112.96±1.25
3.26±1.030.73 >0.05 肝转移 否
是28
223.15±1.14
2.86±1.280.84 >0.05 骨转移 否
是28
223.32±1.08
2.64±1.262.05 < 0.05  下载: 导出CSV
下载: 导出CSV
表 2 ES-SCLC病人基线血清LMR与一线化疗疗效的关系(n)
分组 n PD+SD PR+CR χ2 P 低LMR组 28 18 10 高LMR组 22 7 15 5.20 < 0.05 合计 50 25 25
下载: 导出CSV
表 3 ES-SCLC病人PFS的单因素Cox回归分析
变量 B SE Waldχ2 P HR(95%CI) 性别 -0.842 0.488 2.98 >0.05 0.431(0.165~1.122) 年龄 -0.214 0.361 0.35 >0.05 0.808(0.398~1.638) 吸烟 0.006 0.342 0.00 >0.05 1.006(0.515~1.966) ECOG评分 0.069 0.338 0.04 >0.05 1.071(0.552~2.077) 白蛋白 -0.846 0.453 3.48 >0.05 0.429(0.177~1.044) 肺部炎症 0.048 0.393 0.02 >0.05 1.049(0.485~2.268) 浆膜腔积液 -0.105 0.323 0.11 >0.05 0.900(0.478~1.697) 脏器转移 0.897 0.412 4.74 < 0.05 2.451(1.093~5.496) 脑转移 0.056 0.402 0.02 >0.05 1.057(0.481~2.327) 肝转移 0.411 0.331 1.54 >0.05 1.508(0.788~2.886) 骨转移 -0.608 0.339 3.21 >0.05 0.545(0.280~1.058) LMR -0.722 0.348 4.30 < 0.05 0.486(0.246~0.961)
下载: 导出CSV
表 4 ES-SCLC病人PFS的多因素Cox回归分析
变量 B SE Waldχ2 P HR(95%CI) 脏器转移 0.867 0.408 4.52 < 0.05 2.381(1.070~5.297) LMR -0.698 0.347 4.05 < 0.05 0.498(0.252~0.982)
下载: 导出CSV
表 5 ES-SCLC病人OS的单因素Cox回归分析
变量 B SE Waldχ2 P HR(95%CI) 性别 -1.54 0.524 8.63 < 0.01 0.214(0.077~0.599) 年龄 -0.127 0.395 0.10 >0.05 0.881(0.406~1.910) 吸烟 -0.069 0.355 0.04 >0.05 0.933(0.466~1.871) ECOG评分 0.096 0.354 0.07 >0.05 1.101(0.550~2.205) 白蛋白 -0.381 0.464 0.67 >0.05 0.683(0.275~1.696) 肺部炎症 -0.122 0.439 0.08 >0.05 0.885(0.374~2.092) 浆膜腔积液 -0.364 0.353 1.06 >0.05 0.695(0.348~1.388) 脏器转移 0.869 0.441 3.88 < 0.05 2.384(1.004~5.663) 脑转移 0.126 0.429 0.09 >0.05 1.135(0.490~2.628) 肝转移 0.495 0.37 1.79 >0.05 1.641(0.794~3.388) 骨转移 0.033 0.353 0.01 >0.05 1.034(0.518~2.063) LMR -1.084 0.387 7.86 < 0.01 0.338(0.158~0.722)
下载: 导出CSV
表 6 ES-SCLC病人OS的多因素Cox回归分析
变量 B SE Waldχ2 P HR(95%CI) 性别 -1.253 0.522 5.77 < 0.05 0.286(0.103~0.794) 脏器转移 1.006 0.453 4.94 < 0.05 2.735(1.126~6.644) LMR -1.130 0.406 7.74 < 0.01 0.323(0.146~0.716)
下载: 导出CSV
-
[1] SIEGEL RL, MILLER KD, FUCHS HE, et al. Cancer statistics, 2022[J]. CA Cancer J Clin, 2022, 72(1): 7. doi: 10.3322/caac.21708 [2] XIA C, DONG X, LI H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants[J]. Chin Med J (Engl), 2022, 135(5): 584. doi: 10.1097/CM9.0000000000002108 [3] BERNHARDT EB, JALAL SI. Small cell lung cancer[J]. Cancer Treat Res, 2016, 170: 301. [4] GOLDMAN JW, DVORKIN M, CHEN Y, et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide versus platinum-etoposide alone in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): updated results from a randomised, controlled, open-label, phase 3 trial[J]. Lancet Oncol, 2021, 22(1): 51. doi: 10.1016/S1470-2045(20)30539-8 [5] HORN L, MANSFIELD AS, SZCZESNA A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer[J]. N Engl J Med, 2018, 379(23): 2220. doi: 10.1056/NEJMoa1809064 [6] 柴广金, 李围围, 吕博, 等. PET/CT代谢参数与LMR在评估肺癌放化疗近期疗效的临床研究[J]. 中国CT和MRI杂志, 2021, 19(8): 54. doi: 10.3969/j.issn.1672-5131.2021.08.017 [7] KURAMOCHI H, YAMADA T, YOSHIDA Y, et al. The Pre-treatment lymphocyte-to-monocyte ratio predicts efficacy in metastatic colorectal cancer treated with TAS-102 and bevacizumab[J]. Anticancer Res, 2021, 41(6): 3131. doi: 10.21873/anticanres.15098 [8] MENG X, WANG X, JIANG C, et al. Correlation analysis of lymphocyte-monocyte ratio with pathological complete response and clinical prognosis of neoadjuvant chemotherapy in patients with breast cancer[J]. Transl Oncol, 2022, 18: 101355. doi: 10.1016/j.tranon.2022.101355 [9] GO SI, KIM RB, SONG HN, et al. Prognostic significance of the lymphocyte-to-monocyte ratio in patients with small cell lung cancer[J]. Med Oncol, 2014, 31(12): 323. doi: 10.1007/s12032-014-0323-y [10] 刘建清, 林秀华, 沈志勇. 淋巴细胞与单核细胞比值对晚期肺癌预后预测的价值[J]. 现代肿瘤医学, 2018, 26(11): 1706. doi: 10.3969/j.issn.1672-4992.2018.11.015 [11] QI WX, XIANG Y, ZHAO S, et al. Assessment of systematic inflammatory and nutritional indexes in extensive-stage small-cell lung cancer treated with first-line chemotherapy and atezolizumab[J]. Cancer Immunol Immunother, 2021, 70(11): 3199. doi: 10.1007/s00262-021-02926-3 [12] CHENG Y, FAN Y, LIU X, et al. Randomized controlled trial of lobaplatin plus etoposide vs. cisplatin plus etoposide as first-line therapy in patients with extensive-stage small cell lung cancer[J]. Oncol Lett, 2019, 17(5): 4701. [13] FRIDMAN WH, GALON J, DIEU-NOSJEAN MC, et al. Immune infiltration in human cancer: prognostic significance and disease control[J]. Curr Top Microbiol Immunol, 2011, 344: 1. [14] 麦晓君, 周凤丽. 肺癌微环境细胞分类研究进展[J]. 中国免疫学杂志, 2020, 36(13): 1661. doi: 10.3969/j.issn.1000-484X.2020.13.025 [15] SUZUKI R, LIN SH, WEI X, et al. Prognostic significance of pretreatment total lymphocyte count and neutrophil-to-lymphocyte ratio in extensive-stage small-cell lung cancer[J]. Radiother Oncol, 2018, 126(3): 499. doi: 10.1016/j.radonc.2017.12.030 [16] CAMPIAN JL, YE X, BROCK M, et al. Treatment-related lymphopenia in patients with stage Ⅲ non-small-cell lung cancer[J]. Cancer Invest, 2013, 31(3): 183. doi: 10.3109/07357907.2013.767342 [17] SAITO H, KONO Y, MURAKAMI Y, et al. Prognostic significance of pre- and postoperative lymphocyte counts in patients with gastric cancer[J]. Dig Surg, 2019, 36(2): 137. doi: 10.1159/000486581 [18] TALMOR M, MIRZA A, TURLEY S, et al. Generation or large numbers of immature and mature dendritic cells from rat bone marrow cultures[J]. Eur J Immunol, 1998, 28(3): 811. doi: 10.1002/(SICI)1521-4141(199803)28:03<811::AID-IMMU811>3.0.CO;2-S [19] SCHOPPMANN SF, BIRNER P, STÖCKL J, et al. Tumor-associated macrophages express lymphatic endothelial growth factors and are related to peritumoral lymphangiogenesis[J]. Am J Pathol, 2002, 161(3): 947. doi: 10.1016/S0002-9440(10)64255-1 [20] 吴婧婧, 孙妩弋, 魏伟. 肝细胞癌中M2巨噬细胞标志物与NF-κB p50相关性研究[J]. 蚌埠医学院学报, 2019, 44(4): 421. [21] COUSSENS LM, WERB Z. Inflammation and cancer[J]. Nature, 2002, 420(6917): 860. doi: 10.1038/nature01322 [22] MINAMI S, OGATA Y, IHARA S, et al. Pretreatment Glasgow prognostic score and prognostic nutritional index predict overall survival of patients with advanced small cell lung cancer[J]. Lung Cancer (Auckl), 2017, 8: 249. [23] 许文娟, 马莹, 王译民, 等. 预后营养指数预测小细胞肺癌预后的临床应用研究[J]. 四川大学学报(医学版), 2020, 51(4): 573. [24] KUWADA K, KAGAWA S, YOSHIDA R, et al. The epithelial-to-mesenchymal transition induced by tumor-associated macrophages confers chemoresistance in peritoneally disseminated pancreatic cancer[J]. J Exp Clin Cancer Res, 2018, 37(1): 307. doi: 10.1186/s13046-018-0981-2 [25] 唐和孝, 白玉泉, 申武林, 等. 白介素6在肺癌中的作用研究进展[J]. 浙江大学学报(医学版), 2018, 47(6): 659. [26] MIYAHARA Y, TAKASHI S, SHIMIZU Y, et al. The prognostic impact of neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR) in patients with distal bile duct cancer[J]. World J Surg Oncol, 2020, 18(1): 78. doi: 10.1186/s12957-020-01847-2 [27] MILLER RE, JONES JC, TOMETSKO M, et al. RANKL inhibition blocks osteolytic lesions and reduces skeletal tumor burden in models of non-small-cell lung cancer bone metastases[J]. J Thorac Oncol, 2014, 9(3): 345. doi: 10.1097/JTO.0000000000000070 -

 点击查看大图
点击查看大图

图(2)表(6)
计量
- 文章访问数: 2993
- HTML全文浏览量: 1414
- PDF下载量: 19
- 被引次数: 0
