

 下载:
下载:
-
糖尿病酮症酸中毒(diabetic ketoacidosis,DKA)是胰岛素和反调节激素失衡的结果,以高血糖、高血酮、糖尿、酮尿、脱水、电解质紊乱和代谢性酸中毒为特征[1]。DKA尤其多见于新诊断和确诊1型糖尿病(type 1 diabetes mellitus, T1DM),也可见于2型糖尿病(type 2 diabetes mellitus, T2DM)[1]。近年有证据[2]表明,糖尿病与基因突变有关。本研究对23例新诊断DKA儿童青少年的临床、遗传学和随访资料进行回顾性分析。现作报道。
-
选取2015年11月至2020年3月我院儿科重症监护室住院治疗的23例新诊断DKA患儿为研究对象。均无糖尿病家族史。其中男6例,女17例;年龄0.9~13.7岁,中位年龄10.1岁;农村患儿19例,城镇患儿4例;T1DM 22例(其中糖尿病自身抗体阳性10例),T2DM 1例;轻度DKA 4例,中度DKA 7例,重度DKA 12例。本项目获蚌埠医学院第一附属医院临床医学研究伦理批准通过(批件号: BYYFY-2015KY06)。
-
DKA及其严重度分度参照2018年国际儿童青少年糖尿病协会(ISPAD)临床实践共识指南[1]。糖尿病诊断标准及分型参照中国儿童1型糖尿病标准化诊断与治疗专家共识(2020版)[3]和儿童青少年2型糖尿病诊治中国专家共识[4]。
总结患儿的临床症状和体征。实验室检查: 血常规、尿常规、生化常规、随机血糖(random blood glucose, RBG)、静脉血气、C反应蛋白、糖化血红蛋白(glycated hemoglobin A1c, HbA1c)、C肽、糖尿病自身抗体(谷氨酸脱羧酶抗体、抗胰岛素自身抗体、抗胰岛细胞抗体),根据病情选做降钙素原、细菌培养等。血糖测定采用葡萄糖氧化酶法,HbA1c测定采用离子交换高效液相色谱法,C肽测定采用化学发光法,糖尿病自身抗体测定采用酶联免疫分析法。
-
所有患儿给予补液和小剂量胰岛素持续静脉泵入(0.1 U·kg-1·h-1),DKA纠正后T1DM患儿每天多次胰岛素注射(multiple daily insulin injections, MDI),基础胰岛素采用地特胰岛素,餐时胰岛素采用门冬胰岛素,或持续胰岛素皮下输注(continuous subcutaneous insulin infusion, CSII): 美敦力胰岛素泵或国产微泰EQUIL贴敷式智能胰岛素泵,选用门冬胰岛素;T2DM患儿口服二甲双胍。随访患儿空腹血糖、HbA1c、C肽、糖尿病自身抗体情况。
-
自愿接受基因检查者,抽取外周静脉血2 mL,置于含乙二胺四乙酸抗凝试管,送北京康旭医学检验所进行二代测序,依次经探针设计、基因组DNA文库构建、杂交和捕获、NEXTSEQ 500型测序仪(美国Illumina公司)测序,对有意义的变异进行包括父母在内的一代测序(Sanger测序)验证。采用SIFT(
http://sift.jcvi.org )和Polyphen-2(http://genetics.bwh.harvard.edu/pph2/index.shtml )预测错义变异对蛋白质结构和功能的影响。 -
23例患儿中,烦渴多饮多尿22例,体质量减轻20例,夜尿10例,夜间遗尿2例,呼吸急促16例,腹痛恶心呕吐12例,呼气酮味15例,呼吸深长16例,意识障碍12例,休克15例。合并肺炎1例,急性淋巴细胞白血病(L1型)1例,发热5例,脓毒症3例,肺炎支原体感染6例,泌尿道感染1例。
-
白细胞(WBC)升高16例,其中>10.0×109~20.0×109 /L患儿9例,>20.0×109~30.0×109/L者5例,>30.0×109~40.0×109/L 2例;中性粒细胞比例升高(>70%)13例。中位RBG 25.0 mmol/L(11.48~34.72 mmol/L);平均HbA1c(13.62±2.02)%(9.80%~17.40%);C肽降低22例,平均(0.18±0.09)ng/mL(0.05~0.37 ng/mL);平均静脉pH值为7.06±0.13(6.80~7.23);糖尿病自身抗体阳性10例,重度尿糖(3+~4+)16例,重度尿酮(3+~4+)19例。1例T2DM患儿低密度脂蛋白胆固醇(LDL-C)3.07 mmol/L(>2.6 mmol/L[4])。感染13例,其中C反应蛋白升高6例,降钙素原升高5例,肺炎支原体IgM抗阳性6例,中段尿培养分离出粪肠球菌1例。
-
1例患儿要求转院,余22例抢救成功,平均住院时间12.5 d(3~20 d),平均DKA纠正时间71.0 h(24~136 h)。DKA纠正后T1DM患儿MDI 14例,CSII 8例(美敦力712EWS胰岛素泵4例,712WWL胰岛素泵1例,国产胰岛素泵微泰胰岛素泵3例),1例T2DM患儿口服二甲双胍。
-
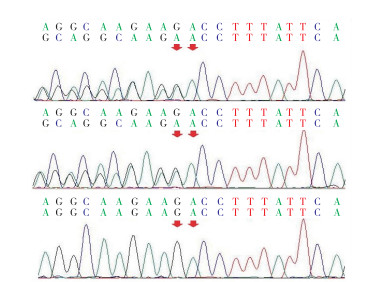
共2例T1DM患儿接受二代测序。其中病例17 PDE11A外显子2存在c.20_21delGA杂合缺失变异(NM_001077197),导致移码突变,提前产生终止密码子,第7位精氨酸(Arg)被苏氨酸(Thr)替换,并在改变后的第30个氨基酸终止(p.Arg7ThrfsTer30)(NP_001070665.1),先证者父亲为野生型,母亲为杂合携带(见图 1)。

图 1 病例17及其家系成员PDE11A基因外显子2测序结果
病例23 PTPN1外显子9存在c.1243G>A杂合错义变异(NM_002827),导致PTPN1蛋白质(NP_002818.1)415位缬氨酸(Val)被蛋氨酸(Met)替换(p.Val415Met),为已报道过的单核苷酸多态性(rs760420089)。SIFT分析显示,p.Val415Met对PTPN1蛋白质影响的预测分数为1.000,Polyphen-2分析显示p.Val415Met对PTPN1蛋白质结构和功能破坏的概率为0.003(敏感性0.98,特异性0.26),提示p.Ala1067Thr对PTPN1蛋白质结构和功能无影响。
-
1例合并白血病患儿出院后4个月死于上消化道大出血,失访4例,余18例平均随访26.5个月(5~57个月),1例T2DM男性患儿空腹血糖5.6 mmol/L,HbA1c 6.8%(起病时15.2%),C肽正常,糖尿病自身抗体阴性,LDL-C 2.77 mmol/L。17例T1DM中位空腹血糖8.06 mmol/L(4.42~26.53 mmol/L),平均HbA1c(8.79±2.20)%(5.5%~14.4%), < 7.0% 3例(17.6%), < 7.5% 6例(35.3%),中位C肽0.09 ng/mL(0.05~0.50 ng/mL),3例T1DM女性患儿分别随访至6、23、25个月时糖尿病自身抗体转阳性。3例T1DM女性患儿随访期间DKA复发。
-
本组23例DKA患儿综合起病和随访确诊T1DM 22例(95.6%),T2DM 1例(4.4%),与文献报道15%~70%的儿童新诊断T1DM和5%~25%的新诊断T2DM以DKA为首发表现基本一致[1]。本组DKA临床表现多样,多饮、多尿、体质量减轻最常见,52.2%的患儿以胃肠道症状为首发表现。本组年龄< 2岁者2例,感染13例,多数为农村家庭患儿(低社会经济状况),父母缺乏糖尿病意识,均无糖尿病家族史,与新诊断DKA危险因素一致[5-6]。HUANG等[7]报道肺炎支原体感染与1例12岁女孩暴发性T1DM有关。本组肺炎支原体感染6例,可能是DKA诱因之一。WBC升高是儿童DKA的应激反应,不能据此判断感染[1]。我们结合发热、C反应蛋白、降钙素原、肺炎支原体IgM抗体、细菌培养和影像学检查综合判断有无感染。
本组22例T1DM患儿起病时和随访中C肽均降低,糖尿病自身抗体阳性13例(59.1%),其中3例系随访中转阳性。糖尿病自身抗体是区分T1DM和T2DM较为准确的方法,然而由于检测方法不一,不能检测到所有糖尿病自身抗体,使其临床价值受限,同时亚洲人群T1DM患儿糖尿病自身抗体阳性率往往较低[4],这些可能是本研究T1DM患儿糖尿病自身抗体阳性率偏低的原因。T2DM患儿系一13.1岁男性患儿,起病时RBG 13.77 mmol/L,HbA1c 15.2%,超重(体质量指数22.8 kg/m2[8])、C肽正常、糖尿病自身抗体阴性、黑棘皮病(后颈部皮肤色素加深)、DKA纠正后不依赖外源性胰岛素治疗,随访中C肽正常,糖尿病自身抗体阴性,起病和随访中存在脂代谢异常(LDL-C升高)。ISPAD临床实践共识指南和美国糖尿病协会分别定义HbA1c< 7.0%[9]和< 7.5%[10]为糖尿病控制目标。本组18例患儿接受随访,1例T2DM患儿HbA1c控制达标,余17例T1DM患儿HbA1c控制达标率低, < 7.0%占17.6%, < 7.5%占35.3%。ISPAD临床实践共识指南指出T1DM以DKA为首发表现是独立于人口学和社会经济状况的预测长期血糖控制不良的危险因素[1],这可能是本组T1DM患儿HbA1c达标率低的主要原因。DKA复发3例,均为T1DM患儿,可能与女性、血糖控制不良、精神心理、低社会经济状况有关[5]。
病例17为T1DM,三多一少症状明显,二代测序显示PDE11A外显子2存在c.20_21delGA杂合缺失变异,导致移码突变,产生一个截短的36个氨基酸残基的蛋白质,而不是正常683个氨基酸的PDE11A蛋白质,经检索人类基因突变数据库(HGMD),c.20_21delGA迄今尚未见报道。家系分析显示c.20_21delGA为遗传性突变,母亲为杂合缺失变异的携带者。PDE11A基因座位于2q31.2,基因组全长492 091 bp,含有24个外显子,PDE11A基因突变与Cushing病和肾上腺皮质增生有关。先证者及其母亲均无Cushing病临床表型,超声无肾上腺皮质增生的证据,PDE11A失活突变可能参与T1DM的发病,有待进一步研究。
综上,儿童青少年新诊断DKA多见于T1DM,临床表现多样,HbA1c达标率低,T1DM可能与PDE11A基因突变有关。
儿童青少年新诊断糖尿病酮症酸中毒临床、遗传学及随访分析
Clinical, genetic and follow-up analysis of newly diagnosed diabetic ketoacidosis in children and adolescents
-
摘要:
目的分析儿童青少年新诊断糖尿病酮症酸中毒(DKA)的临床表现、遗传学及随访结局。 方法回顾分析23例DKA患儿的临床和随访资料,自愿接受基因检查者给予二代测序。 结果男6例,女17例,中位年龄10.1岁。1型糖尿病(T1DM)22例,2型糖尿病(T2DM)1例。烦渴多饮多尿22例,呼吸深长16例,腹痛恶心呕吐12例,发热5例,意识障碍12例,休克15例。中位随机血糖25.0 mmol/L(11.48~34.72 mmol/L),平均糖化血红蛋白13.62%(9.80%~17.40%),C肽降低22例,平均0.18 ng/mL(0.05~0.37 ng/mL),平均静脉pH 7.06(6.80~7.23),糖尿病自身抗体阳性10例。所有患儿给予补液、小剂量胰岛素持续静脉泵入治疗,1例转院,22例抢救成功。DKA纠正后T1DM患儿给予胰岛素治疗,T2DM患儿口服二甲双胍。随访18例,平均随访26.5月(5~57个月),1例T2DM患儿HbA1c 6.8%,17例T1DM患儿平均HbA1c 8.79%(5.5%~14.4%),中位C肽0.09 ng/mL(0.05~0.50 ng/mL),3例T1DM患儿糖尿病自身抗体转阳性。2例T1DM患儿接受二代测序,其中1例PDE11A外显子2存在c.20_21delGA杂合缺失变异,导致阅读框改变,蛋白质截短(p.Arg7ThrfsTer30),父亲为野生型,母亲为杂合携带。 结论儿童青少年新诊断DKA多见于T1DM,临床表现多样,HbA1c达标率低,PDE11A基因突变可能与T1DM有关。 Abstract:ObjectiveTo analyze the clinical features, genetics and follow-up outcomes of newly diagnosed diabetic ketoacidosis(DKA) in children and adolescents. MethodsThe clinical and follow-up data of 23 newly diagnosed DKA patients were retrospectively analyzed.Those who were willing to undergo gene examination were given second-generation sequencing. ResultsAmong the 23 patients, there were 6 males and 17 females with a median age of 10.1 years.There were 22 cases of type 1 diabetes mellitus(T1DM) and 1 case of type 2 diabetes mellitus(T2DM).There were 22 cases of polydipsia, 16 cases of prolonged breathing, 12 cases of abdominal pain, nausea and vomiting, 5 cases of fever, 12 cases of disturbance of consciousness and 15 cases of shock.The median random blood glucose was 25.0 mmol/L(11.48-34.72 mmol/L), and the mean HbA1c was 13.62%(9.80%-17.40%).The C peptide decreased in 22 cases, the level of which was 0.18 ng/mL(0.05-0.37 ng/mL).The mean of venous pH was 7.06(6.80-7.23), and the diabetes autoantibody in 10 patients were positive.All children were treated with fluid rehydration and continuous intravenous pumping of low-dose insulin.One case was transferred to hospital, and 22 cases were successfully rescued.After DKA correction, T1DM patients were treated with insulin, and T2DM patients were treated with metformin orally.Eighteen patients were followed up for an average of 26.5 months(5-57 months).The HbA1c was 6.8% in 1 patient with T2DM, and 8.79%(5.5%-14.4%) in 17 patients with T1DM.The median C-peptide was 0.09 ng/mL(0.05-0.50 ng/mL).The diabetes autoantibody in 3 T1DM children were positive.The second-generation sequencing in two children with T1DM were performed, the c.20_21delGA heterozygous deletion mutation in exon 2 of PDE11A in 1 cases was found, which leaded to the reading frame changes and protein truncation(p.Arg7ThrfsTer30).The father was wild-type, and the mother was heterozygous carrier. ConclusionsThe newly diagnosed DKA in children and adolescents is mostly found in T1DM, with various clinical manifestations and low HbA1c compliance rate.The PDE11A gene mutation may be related to T1DM. -
Key words:
- diabetic ketoacidosis /
- gene /
- child /
- adolescent
-
[1] WOLFSDORF JI, GLASER N, AGUS M, et al. ISPAD Clinical Practice Consensus Guidelines 2018: diabetic ketoacidosis and the hyperglycemic hyperosmolar state[J]. Pediatr Diabetes, 2018, 19 Suppl 27: 155. [2] MAYER-DAVIS EJ, KAHKOSKA AR, JEFFERIES C, et al. ISPAD Clinical Practice Consensus Guidelines 2018: definition, epidemiology, and classification of diabetes in children and adolescents[J]. Pediatr Diabetes, 2018, 19(Suppl 27): 7. [3] 中华医学会儿科学分会内分泌遗传代谢学组, 中华儿科杂志编辑委员会. 中国儿童1型糖尿病标准化诊断与治疗专家共识(2020版)[J]. 中华儿科杂志, 2020, 58(6): 447. doi: 10.3760/cma.j.cn112140-20200221-00124 [4] 中华医学会儿科学分会内分泌遗传代谢学组. 儿童青少年2型糖尿病诊治中国专家共识[J]. 中华儿科杂志, 2017, 55(6): 404. doi: 10.3760/cma.j.issn.0578-1310.2017.06.002 [5] JEFFERIES CA, NAKHLA M, DERRAIK JG, et al. Preventing diabetic ketoacidosis[J]. Pediatr Clin North Am, 2015, 62(4): 857. doi: 10.1016/j.pcl.2015.04.002 [6] USHER-SMITH JA, THOMPSON MJ, SHARP SJ, et al. Factors associated with the presence of diabetic ketoacidosis at diagnosis of diabetes in children and young adults: a systematic review[J]. BMJ, 2011, 343: d4092. doi: 10.1136/bmj.d4092 [7] HUANG Z, XU L, LI F, et al. Fulminant type 1 diabetes mellitus with rhabdomyolysis: have we overlooked the situation?[J]. Diabetes Res Clin Pract, 2010, 90(3): e47. doi: 10.1016/j.diabres.2010.07.010 [8] 李辉, 季成叶, 宗心南, 等. 中国0~18岁儿童、青少年体块指数的生长曲线[J]. 中华儿科杂志, 2009, 47(7): 493. doi: 10.3760/cma.j.issn.0578-1310.2009.07.004 [9] DIMEGLIO LA, ACERINI CL, CODNER E, et al. ISPAD Clinical Practice Consensus Guidelines 2018: glycemic control targets and glucose monitoring for children, adolescents, and young adults with diabetes[J]. Pediatr Diabetes, 2018, 19(Suppl 27): 105. [10] American Diabetes Association. Children and Adolescents: Standards of Medical Care in Diabetes-2018[J]. Diabetes Care, 2018, 41(Suppl 1): S126. -

 点击查看大图
点击查看大图
图(1)
计量
- 文章访问数: 1790
- HTML全文浏览量: 790
- PDF下载量: 9
- 被引次数: 0
