

-
肝细胞癌(hepatocellular carcinoma, HCC)占原发性肝癌的75%~85%[1],其中50%的死亡病例出现在中国,是我国发病率第四位的恶性肿瘤[2]。HCC发病率高,死亡率高,严重威胁人类健康。目前HCC的诊断和治疗水平有了明显提高,手术仍为首选治疗。但术后复发率高,预后仍不容乐观[3]。
HCC是高度血管化的肿瘤。血管生成在HCC的发生和发展过程中起重要作用[4]。血管内皮生长因子(vascular endothelial growth factor, VEGF)在血管生成中发挥重要作用,在多种肿瘤中均有表达,并影响肿瘤病人预后[5-6]。同源盒基因是一个转录编码家族,同源盒基因B7(homeobox B7, HOXB7)是同源盒基因家族的成员,作为重要的转录因子,HOXB7能够调节癌细胞的多种功能,包括增殖、侵袭、迁移、血管生成和上皮-间质转化(EMT)[7]。此外,HOXB7的过表达与癌症进展和不良预后显著相关[8]。
在临床工作中我们发现影响HCC病人术后预后的因素不仅有临床因素,还与病理因素息息相关,因此,本研究中我们利用免疫组织化学分析研究了VEGF和HOXB7两种分子标志物对术后HCC病人预后的影响。
-
选取2011-2014年在唐山市人民医院进行手术治疗的74例HCC病人,所有病人均有明确的病理诊断,并且有术后石蜡标本。临床资料统计病人术前甲胎蛋白(AFP)的水平、Child-Pugh分级、术前是否经射频消融(RFA)或经动脉化学栓塞(TACE)治疗、手术类型和疾病复发时间。病理学资料包括肿瘤的大小和数量,被膜侵犯和病理分级。使用根据国际肿瘤分类学(ICD-O)进行病理分级[9]。根据美国癌症联合委员会(AJCC)分类系统进行TNM分期[10],本研究经唐山市人民医院伦理委员会审查和批准。
-
将石蜡标本制成5 μm厚切片,常规二甲苯脱蜡、乙醇水化,使用3%过氧化氢的甲醇溶液抑制内源性过氧化物酶。滴加正常山羊血清封闭,室温封闭20 min。分别滴加鼠抗人HOXB7单克隆抗体,鼠抗人VEGF单克隆抗体,4 ℃冰箱孵育过夜。用PBS冲洗3次后,滴加生物素标记的二抗室温孵育30 min,DAB显色,常规复染、脱水、透明和封片。以未经免疫的兔血清代替一抗染色作为阴性对照(本试验一抗购自美国Santa Cruz Biotechnology公司,其余试剂均购自北京中杉金桥公司)。TE2000-u倒置生物显微镜(日本Nikon公司)观察切片。
-
使用组织评分系统对结果进行定量。通过将阳性细胞的百分比乘以染色强度来确定组织得分。根据染色强度等级评分(0,不染色;1,弱染色;2,中度染色;3,强染色)。根据染色细胞的百分比评分(0,无染色细胞;1, < 5%;2,≥5%~25%;3,>25%~50%;4,>50%~75%;5,>75%的染色细胞)。计算最终得分为染色强度乘以相应区域中染色细胞百分比。将最终得分归类如下: 0,阴性(-);1~4,弱阳性(+);5~9,中度阳性2+;10~15,强阳性3+[11]。
-
采用χ2检验和Cox风险比例模型。
-
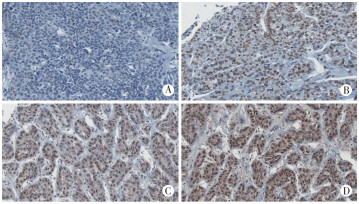
74例病人中,男58例,女16例,年龄33~75岁。Child-Pugh分级: A级64例,B级10例。74例病人中62例为HBV感染(83.8%),4例为HCV感染(5.4%),6例为酒精性肝硬化(8.1%)。肿瘤大小为0.9~11 cm。57例(77.0%)病人为单个肿瘤,16例(21.6%)病人有2个肿瘤,1例(1.4%)病人有3个肿瘤。根据ICD-O进行病理分级,Ⅰ级12例(16.2%),Ⅱ级27例(36.5%),Ⅲ级33例(44.6%),Ⅳ级2例(2.7%)。根据AJCC进行肿瘤分期[9]: T1期43例(58.1%),T2期22例(29.7%),T3期9例(12.1%)。VEGF在肿瘤细胞中主要为细胞质染色(见图 1)。HOXB7在肿瘤细胞中主要为细胞核和胞质染色(见图 2)。两者的表达情况见表 1。

图 1 肝细胞癌中VEGF的表达

图 2 肝细胞癌中HOXB7的表达
阴性 弱阳性 中等阳性 强阳性 VEGF 32(43.2) 15(20.3) 22(29.7) 5(6.8) HOXB7 14(18.9) 36(48.6) 19(25.7) 5(6.8) 表 1 HCC病人VEGF和HOXB7免疫组织化学染色结果[n; 百分率(%)]
-
74例病人术后5年总生存率分别为48.6%。单因素分析表明,不同性别、年龄和肿瘤病理分级的HCC病人的5年生存率差异无统计学意义(P>0.05)。不同Child-Pugh分级、T分期、肿瘤直径、AFP表达、被膜侵犯及肿瘤个数的病人5年生存率差异有统计学意义(P < 0.01)。单因素分析显示,VEGF和HOXB7表达水平,与HCC病人生存期相关。生存分析表明,VEGF表达水平较高病人的5年生存率明显低于VEGF表达水平较低的病人(P < 0.05)。HOXB7表达水平较高的病人总体生存率明显低于HOXB7表达水平较低的病人(P < 0.05)(见表 2)。
参数 n 5年生存人数 χ2 P 性别 男
女58
1628(48.3)
8(50.0)0.02 >0.05 年龄/岁 ≤60
>6057
1726(45.6)
10(58.8)0.91 >0.05 Child-Pugh分级 A
B64
1035(54.7)
1(10.0)6.91 < 0.01 AFP/(ng/mL) ≤400
>40052
2229(55.8)
7(31.8)3.55 < 0.05 肿瘤直径/cm ≤5
>565
935(53.8)
1(11.1)5.78 < 0.05 肿瘤个数 1
≥257
1743(75.4)
2(11.8)22.28 < 0.01 T分期 T1、T2
T365
935(53.8)
1(11.1)5.78 < 0.05 被膜侵犯 阴性
阳性56
1831(55.4)
6(33.3)2.64 >0.05 病理分级 Ⅰ 12 11(91.7) Ⅱ
Ⅲ27
3322(81.5)
3(9.1)43.11 < 0.01 Ⅳ 2 0(0.0) VEGF -、+
2+、3+47
2728(59.6)
8(29.6)6.16 < 0.05 HOXB7 -、+
2+、3+50
2428(56.0)
6(25.0)6.28 < 0.05 表 2 影响HCC病人预后的临床病理和免疫组织化学因素[n; 百分率(%)]
-
使用Cox比例风险模型对影响HCC病人术后总体生存的预后因素进行多变量分析, 结果显示Child-Pugh分级、T分期、肿瘤个数、HOXB7表达和VEGF表达为影响HCC病人术后生存的独立危险因素(P < 0.01)(见表 3)。
变量 分组 B SE Waldχ2 P HR(95%CI) Child-Pugh分级 A
B1.411 0.422 11.182 < 0.01 4.100(1.793~9.374) T分期 T1、T2
T31.479 0.268 30.544 < 0.01 4.317(2.597~7.413) 肿瘤个数 1
≥20.970 0.422 11.182 < 0.01 2.639(1.364~5.105) HOXB7 -、+
2+、3+0.130 0.042 9.669 < 0.01 1.139(1.049~1.236) VEGF -、+
2+、3+1.326 0.346 18.432 < 0.01 1.192(1.106~1.285) 表 3 影响HCC病人总体生存的预后因素的多变量分析
-
近年来得益于靶向药物的出现以及外科技术的发展, 肝癌病人的生存期有了明显提高[12]。但是目前HCC病人因为缺少有效的术后辅助治疗手段[13],术后复发率仍然很高[14]。本研究中,我们通过分析临床病理资料和免疫组化结果, 发现Child-Pugh分级、肿瘤个数、VEGF和HOXB7的表达是影响HCC病人术后生存的重要因素。HCC病人术后复发是影响病人生存的主要因素[6]。通过对临床和病理资料的分析, 发现Child-Pugh分级、T分期、肿瘤直径、AFP表达水平、被膜侵犯、肿瘤个数与HCC病人术后的生存率相关。
肿瘤血管生成是影响肿瘤预后的重要因素[5-6, 15]。肿瘤血管生成涉及一系列细胞因子,其中影响肿瘤血管生成作用最强的血管生成因子就是VEGF[16-17]。HCC是高度血管化的肿瘤。多项研究表明VEGF在HCC中对预后有影响[18-19]。在HCC病人中,新生血管往往伴随着肿瘤的微浸润[5]。本研究中,VEGF高表达组5年生存率显著低于低表达组,这可能与肿瘤血管新生造成肿瘤微浸润微有关[20]。目前临床常规检查手段很难预测肿瘤微浸润的存在。因此检测VEGF表达可以为病人预后的预测提供一定帮助。有研究表明影响HCC术前肿瘤微浸润的因素中,血清AFP水平>400 mg/L,总肿瘤直径>5 cm,肿瘤多发是肿瘤微浸润的预测因素[21], 这与本研究的结果一致。肿瘤组织中VEGF的表达对病人预后有影响,VEGF水平高表达预示较差的生存期(HR=1.192,95%CI=1.106~1.285)。VEGF水平似乎是评估HCC病人总体生存的重要预后因素。有研究表明,高VEGF表达的病人具容易出现肝脏被膜侵犯,血管浸润和肝内转率,从而表明高VEGF表达的肿瘤在临床上具有侵袭性[22]。
同源盒基因家族包含39个成员,分为四个组(A、B、C、D),调节胚胎发育、生长分化、细胞凋亡和血管生成的信号通路[23]。同源盒基因编码一系列转录因子,这些转录因子对于调节胚胎发育过程中的生长和分化以及维持分化成熟组织的稳态是必不可少的。而这些转录因子的失调影响肿瘤细胞增殖,侵袭和凋亡[7]。HOXB7是同源盒基因家族的成员,HOXB7过表达影响胃癌[24]、食管癌[25]、胰腺癌病人的生存[26]。研究表明HOXB7可调节肝癌细胞增殖和迁移,其高表达与肝癌病人预后相关[27]。本研究中,免疫组织化学分析显示,HOXB7的表达是手术切除后HCC病人生存的重要预后因素(HR=1.139,95%CI=1.049~1.236)。HOXB7的过表达促进HCC细胞增殖和迁移,与VEGF协同作用促进肿瘤血管生成,影响HCC病人生存[27]。
综上所述,在进行手术治疗的HCC病人中,HCC病人Child-Pugh分级、T分期、肿瘤大小、AFP表达水平、被膜侵犯、肿瘤个数是影响病人生存率的重要因素。HCC组织高表达VEGF和HOXB7是HCC病人预后不良的因素。VEGF和HOXB7可以作为HCC病人预后的预测指标。
HOXB7和VEGF对肝细胞癌病人预后影响的研究
Effect of HOXB7 and VEGF on the prognosis of patients with HCC
-
摘要:
目的通过研究肝细胞癌病人同源盒基因B7(HOXB7)和血管内皮生长因子(VEGF)的表达,探讨其对肝细胞癌病人术后预后的影响。 方法收集74例肝细胞癌病人临床病理和生存数据,应用免疫组织化学对术后病理标本进行HOXB7和VEGF染色。分析影响病人预后的因素。 结果74例病人术后3年和5年总生存率分别为67.6%和48.6%。多因素分析显示,HOXB7(P < 0.01, HR=1.139),VEGF(P < 0.01, HR=1.192)、Child-Pugh分级(P < 0.01, HR=4.100)、T分期(P < 0.01, HR=4.317)、肿瘤数量(P < 0.01, HR=2.639)是影响病人生存的独立危险因素。免疫组织化学染色显示,HOXB7和VEGF表达影响病人5年生存率。 结论HOXB7和VEGF过表达影响肝细胞癌病人生存率和预后,是预后不良的因素。 Abstract:ObjectiveTo investigate the effect of homeobox B7 (HOXB7) and vascular endothelial growth factor(VEGF) expressions on the prognosis of patients with hepatocellular carcinoma(HCC) after operation. MethodsSeventy-four patients with HCC following surgical resection were enrolled.Clinicopathological and survival data were analyzed, and immunohistochemical staining method for HOXB7 and VEGF expressions measurement was performed on tissue microarray sections. ResultsThe 3-and 5-year overall survival rates in the 74 patients were 67.6% and 48.6%, respectively.Multivariate analysis revealed that HOXB7(P < 0.01, HR=1.139) and VEGF(P < 0.01, HR=1.192) expressions, Child-Pugh class(P < 0.01, HR=4.100), T stage(P < 0.01, HR=4.317), Tumor number(P < 0.01, HR=2.639) were the independent prognostic factors for overall survival rate.Immunohistochemical staining results showed that the expressions of HOXB7 and VEGF influenced the 5-year survival rate. ConclusionsHOXB7 and VEGF overexpression affect the survival and prognosis of HCC patients, which suggesting a poor overall survival rate. -
Key words:
- heputocellular carcinoma /
- homeobox B7 /
- vascular endothelial growth factor /
- prognosis /
- survival rate
-
表 1 HCC病人VEGF和HOXB7免疫组织化学染色结果[n; 百分率(%)]
阴性 弱阳性 中等阳性 强阳性 VEGF 32(43.2) 15(20.3) 22(29.7) 5(6.8) HOXB7 14(18.9) 36(48.6) 19(25.7) 5(6.8)  下载: 导出CSV
下载: 导出CSV
表 2 影响HCC病人预后的临床病理和免疫组织化学因素[n; 百分率(%)]
参数 n 5年生存人数 χ2 P 性别 男
女58
1628(48.3)
8(50.0)0.02 >0.05 年龄/岁 ≤60
>6057
1726(45.6)
10(58.8)0.91 >0.05 Child-Pugh分级 A
B64
1035(54.7)
1(10.0)6.91 < 0.01 AFP/(ng/mL) ≤400
>40052
2229(55.8)
7(31.8)3.55 < 0.05 肿瘤直径/cm ≤5
>565
935(53.8)
1(11.1)5.78 < 0.05 肿瘤个数 1
≥257
1743(75.4)
2(11.8)22.28 < 0.01 T分期 T1、T2
T365
935(53.8)
1(11.1)5.78 < 0.05 被膜侵犯 阴性
阳性56
1831(55.4)
6(33.3)2.64 >0.05 病理分级 Ⅰ 12 11(91.7) Ⅱ
Ⅲ27
3322(81.5)
3(9.1)43.11 < 0.01 Ⅳ 2 0(0.0) VEGF -、+
2+、3+47
2728(59.6)
8(29.6)6.16 < 0.05 HOXB7 -、+
2+、3+50
2428(56.0)
6(25.0)6.28 < 0.05
下载: 导出CSV
表 3 影响HCC病人总体生存的预后因素的多变量分析
变量 分组 B SE Waldχ2 P HR(95%CI) Child-Pugh分级 A
B1.411 0.422 11.182 < 0.01 4.100(1.793~9.374) T分期 T1、T2
T31.479 0.268 30.544 < 0.01 4.317(2.597~7.413) 肿瘤个数 1
≥20.970 0.422 11.182 < 0.01 2.639(1.364~5.105) HOXB7 -、+
2+、3+0.130 0.042 9.669 < 0.01 1.139(1.049~1.236) VEGF -、+
2+、3+1.326 0.346 18.432 < 0.01 1.192(1.106~1.285)
下载: 导出CSV
-
[1] LIU HZ, DENG W, LI JL, et al. Peripheral blood lymphocyte subset levels differ in patients with hepatocellular carcinoma[J]. Oncotarget, 2016, 7(47): 77558. doi: 10.18632/oncotarget.13041 [2] ZHOU M, WANG H, ZENG X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2019, 394(10204): 1145. doi: 10.1016/S0140-6736(19)30427-1 [3] BRAY F, FERLAY J, SOERJOMATARAM I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2018, 68(6): 394. doi: 10.3322/caac.21492 [4] VERSMISSEN J, MIRABITO COLAFELLA KM, KOOLEN SLW, et al. Vascular cardio-oncology: vascular endothelial growth factor inhibitors and hypertension[J]. Cardiovasc Res, 2019, 115(5): 904. doi: 10.1093/cvr/cvz022 [5] NG KK, CHEUNG TT, PANG HH, et al. A simplified prediction model for early intrahepatic recurrence after hepatectomy for patients with unilobar hepatocellular carcinoma without macroscopic vascular invasion: an implication for adjuvant therapy and postoperative surveillance[J]. Surg Oncol, 2019, 30: 6. doi: 10.1016/j.suronc.2019.05.017 [6] LI Z, LEI Z, XIA Y, et al. Association of preoperative antiviral treatment with incidences of microvascular invasion and early tumor recurrence in hepatitis b virus-related hepatocellular carcinoma[J]. JAMA Surg, 2018, 153(10): e182721. doi: 10.1001/jamasurg.2018.2721 [7] JOO MK, PARK JJ, YOO HS, et al. The roles of HOXB7 in promoting migration, invasion, and anti-apoptosis in gastric cancer[J]. J Gastroenterol Hepatol, 2016, 31(10): 1717. doi: 10.1111/jgh.13330 [8] ERRICO MC, JIN K, SUKUMAR S, et al. The widening sphere of influence of HOXB7 in solid tumors[J]. Cancer Res, 2016, 76(10): 2857. doi: 10.1158/0008-5472.CAN-15-3444 [9] FRITZ A. PCJA. International classification of diseases for oncology(ICD-O) 3rd[Z]. 2000. [10] Edge Sb BDCC. AJCC Cancer Staging Manual. 7th[Z]. New York: Springer: 2009. [11] MEGO M, CIERNA Z, SVETLOVSKA D, et al. PARP expression in germ cell tumours[J]. J Clin Pathol, 2013, 66(7): 607. doi: 10.1136/jclinpath-2012-201088 [12] FAN ST, MAU LC, POON RT, et al. Continuous improvement of survival outcomes of resection of hepatocellular carcinoma: a 20-year experience[J]. Ann Surg, 2011, 253(4): 745. doi: 10.1097/SLA.0b013e3182111195 [13] KIM DY, AHN SH, KIM SU, et al. Adjuvant hepatic arterial infusional chemotherapy with 5-fluorouracil and cisplatin after curative resection of hepatocellular carcinoma[J]. Oncology, 2011, 81(3/4): 184. [14] MENICONI RL, KOMATSU S, PERDIGAO F, et al. Recurrent hepatocellular carcinoma: a Western strategy that emphasizes the impact of pathologic profile of the first resection[J]. Surgery, 2015, 157(3): 454. doi: 10.1016/j.surg.2014.10.011 [15] 肖磊, 邢树山, 郭智珍, 等. CXCL12和VEGF与造釉细胞型颅咽管瘤复发的相关性研究[J]. 中国煤炭工业医学杂志, 2017, 20(9): 1064. [16] LEUNG DW, CACHIANES G, KUANG WJ, et al. Vascular endothelial growth factor is a secreted angiogenic mitogen[J]. Science, 1989, 246(4935): 1306. doi: 10.1126/science.2479986 [17] 邢树山, 刘文庆, 胡万宁, 等. uPA和VEGF与儿童造釉细胞型颅咽管瘤复发的相关性研究[J]. 中华神经外科杂志, 2013, 29(6): 561. [18] CHOI SB, HAN HJ, KIM WB, et al. VEGF overexpression predicts poor survival in hepatocellular carcinoma[J]. Open Med(Wars), 2017, 12: 430. doi: 10.1515/med-2017-0061 [19] DAI W, WANG Y, YANG T, et al. Downregulation of exosomal CLEC3B in hepatocellular carcinoma promotes metastasis and angiogenesis via AMPK and VEGF signals[J]. Cell Commun Signal, 2019, 17(1): 113. doi: 10.1186/s12964-019-0423-6 [20] MEI Z, JIAO H, WANG W, et al. Polycomb chromobox 4 enhances migration and pulmonary metastasis of hepatocellular carcinoma cell line MHCC97L[J]. Sci China Life Sci, 2014, 57(6): 610. doi: 10.1007/s11427-014-4663-9 [21] ZHAO WC, FAN LF, YANG N, et al. Preoperative predictors of microvascular invasion in multinodular hepatocellular carcinoma[J]. Eur J Surg Oncol, 2013, 39(8): 858. doi: 10.1016/j.ejso.2013.04.003 [22] AHMAD NS, MARTIN SG, STORR SJ. Immunohistochemical assessment of leukocyte involvement in angiogenesis[J]. Methods Mol Biol, 2016, 1430: 49. [23] SU J, HUANG YH, CUI X, et al. Homeobox oncogene activation by pan-cancer DNA hypermethylation[J]. Genome Biol, 2018, 19(1): 108. doi: 10.1186/s13059-018-1492-3 [24] TU W, ZHU X, HAN Y, et al. Overexpression of HOXB7 is associated with a poor prognosis in patients with gastric cancer[J]. Oncol Lett, 2015, 10(5): 2967. doi: 10.3892/ol.2015.3630 [25] LI H, SHEN LY, YAN WP, et al. Deregulated HOXB7 expression predicts poor prognosis of patients with esophageal squamous cell carcinoma and regulates cancer cell proliferation in vitro and in vivo[J]. PLoS One, 2015, 10(6): e130551. [26] NGUYEN KA, ARENSMAN M, LAY AR, et al. HOXB7 promotes invasion and predicts survival in pancreatic adenocarcinoma[J]. Cancer, 2013, 119(3): 529. doi: 10.1002/cncr.27725 [27] HUAN H, YANG D, WEN X, et al. HOXB7 accelerates the malignant progression of hepatocellular carcinoma by promoting stemness and epithelial-mesenchymal transition[J]. J Exp Clin Cancer Res, 2017, 36(1): 86. doi: 10.1186/s13046-017-0559-4 -

 点击查看大图
点击查看大图

图(2)表(3)
计量
- 文章访问数: 2613
- HTML全文浏览量: 1456
- PDF下载量: 5
- 被引次数: 0
