


-
脊髓型颈椎病(CSM)是主要的颈椎病类型之一,若无手术禁忌证一经确诊建议尽早开展手术治疗,以使受压的神经、脊髓获得彻底减压,恢复节段稳定性以及正常的颈椎生理曲度,避免脊髓损伤进一步加重。但其手术方式仍存在诸多争议,尤其是多节段患病者,报道称,对以椎管狭窄为主的多节段颈椎病进行后路椎管成形术治疗的临床疗效是确切的,且手术损伤明显轻于前路手术,建议≥3个节段患病的颈椎病病人开展后路手术治疗[1]。目前关于多节段CSM椎管扩大成形术疗效的影响因素多集中在手术减压彻底性、手术入路选择等方面,由于缺少进行术前脊髓受压影像特点的量化工具,既往对以术前影像学参数为主的自身影响因素的报道较少[2]。为进一步明确多节段CSM椎管扩大成形术疗效的影响因素,现纳入120例病人进行手术疗效的危险因素分析。现作报道。
-
选择2016年12月至2018年12月120例多节段CSM病人为研究对象,均采用椎管扩大成形术治疗,随访1~3年,末次随访采用日本骨科协会(JOA)评分评价临床疗效,并设为由优良组与可差组。其中男69例,女51例;年龄36~74岁;患病节段: C2~C5 10例,C3~C6 35例,C4~C7 43例;C2~C6 10例,C3~C7 22例。纳入标准: ≥3连续节段受累的CSM;均接受后路单开门椎管扩大成形术;影像资料以及一般资料完整;随访时间>1年;无颈椎骨折史、外科手术治疗史。排除标准: 合并严重的颈椎肿瘤、结核、后纵韧带骨化;先天性脊柱侧凸、后凸畸形;合并脑血管疾病、中枢神经疾病等影响肢体功能。
-
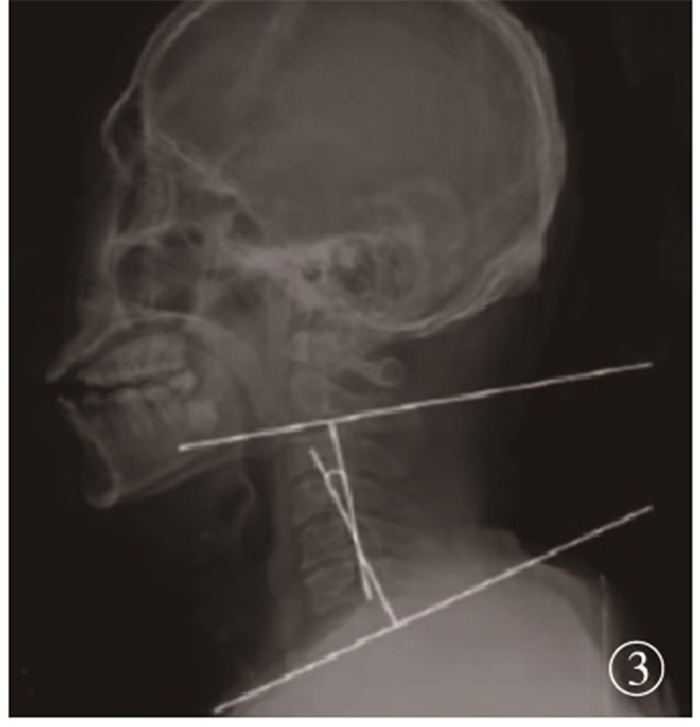
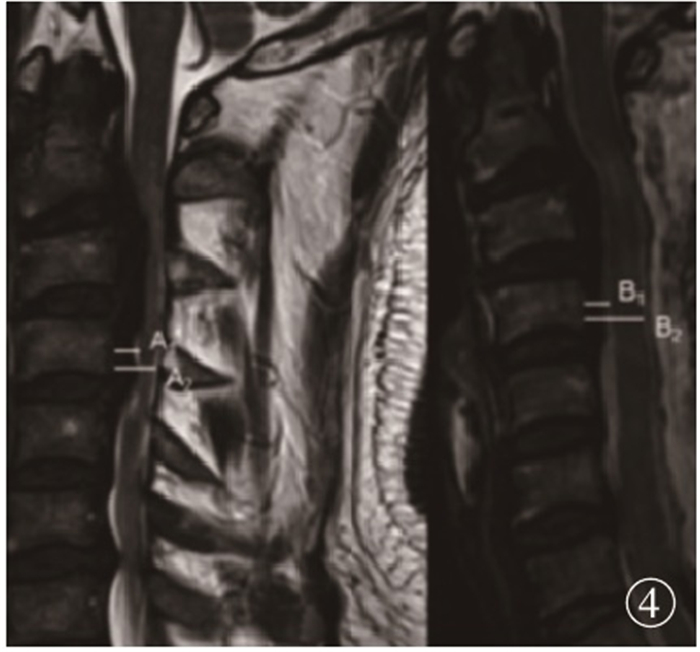
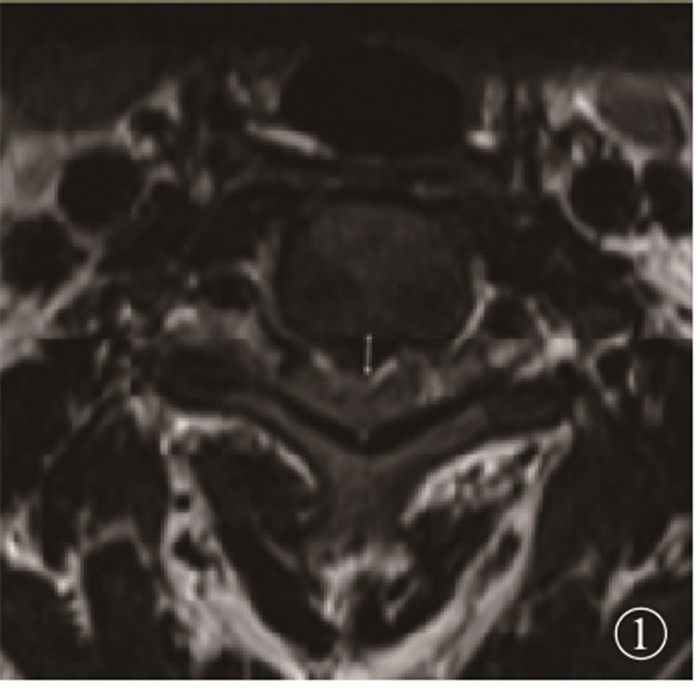
采用JOA评分[3]评价手术疗效,包括下肢运动能力、膀胱功能、感觉功能以及上肢活动能力,总分17分,分值越高提示颈椎功能越良好;以JOA评分改善率评价临床疗效,即术后、术前评分差值与总分、术前评分的差值比值,JOA评分改善率≥75%、50%~74%、25%~49%、 < 25%分别判定为手术疗效优、良、可、差,并设为由优良组与可差组。影像参数调查[4]: 收集手术前后CT、MRI以及侧位X线片。致压物最大径: 术前MRI T2加权横断面图进行测量(见图 1A); 平均压迫率: MRI T2加权正中矢状位患病节段内各致压物矢状径与椎管矢状径之和的比值(见图 1B);术前Cobb角: 颈椎侧位X线片上做C2、C7椎体下终板垂线,两垂线夹角为Cobb角(见图 1C);脊髓漂移距离: 手术前后患病节段脊髓中点与椎后缘距离,即(A1+A2)/2与(B1+B2)/2,脊髓漂移距离=两者差值的1/2(见图 1D)。组间通过单因素及多因素分析调查影响疗效的独立影响因素,即以单因素分析中差异具有统计学意义的项目为自变量,手术优良与可差为因变量进行多因素logistic回归分析。

图 1 术前MRI T2加权横断面图像下测量致压物最大径

图 2 MRI T2加权矢状位图像计算平均压迫率,即(a+b+c+d+e)/(A+B+C+D+E)

图 3 侧位X线片计算Cobb角

图 4 MRI T2加权矢状位图像计算脊髓漂移距离
-
采用χ2检验和多因素logistic回归分析。
-
120例病人末次随访疗效评价优34例,良61例,可20例,差5例,优良率79.17%;2组病程、年龄、致压物最大径、平均压迫率、脊髓漂移距离、术前Cobb角、术前JOA评分差异均有统计学意义(P < 0.05~P < 0.01);2组性别、患病节段数差异均无统计学意义(P>0.05)(见表 1)。
因素 优良组(n=95) 可差组(n=25) χ2 P 病程/年 < 1 59 7 1~2 25 10 5.83 < 0.05 > 2 11 8 年龄/岁 ≤60 74 13 6.66 < 0.05 > 60 21 12 术前JOA评分/分 < 10 20 11 4.75 < 0.05 ≥10 75 14 性别 男 54 15 0.08 > 0.05 女 41 10 患病节段数 三节段 71 17 0.46 > 0.05 四节段 24 8 致压物最大径/mm > 5 80 15 7.03 < 0.05 ≤5 15 10 平均压迫率/% > 30 70 13 4.36 < 0.05 ≤30 25 12 脊髓漂移距离/mm < 2.6 15 9 5.05 < 0.05 ≥2.6 80 16 术前Cobb角/(°) > 10 65 11 5.08 < 0.05 ≤10 30 14 表 1 多节段CSM椎管扩大成形术疗效单因素分析
影响因素 B SE Waldχ2 P OR(95%CI) 病程>2年 0.911 0.306 8.89 < 0.05 2.487(1.431~7.786) 致压物最大径>5 mm 1.135 0.310 13.41 < 0.05 3.112(1.265~12.271) 脊髓漂移距离 < 2.6 mm 0.913 0.307 8.88 < 0.05 2.439(1.176~7.471) 平均压迫率>30% 1.107 0.324 11.68 < 0.05 3.026(1.519~8.080) 术前JOA评分 < 10分 1.047 0.321 10.65 < 0.05 2.855(1.640~11.232) 表 2 多节段CSM椎管扩大成形术疗效多因素分析
-
多因素logistic回归分析显示,病程>2年、致压物最大径>5 mm、脊髓漂移距离 < 2.6 mm、平均压迫率>30%、术前JOA评分 < 10分是影响多节段CSM椎管扩大成形术疗效的独立危险因素(P < 0.05)(见表 2)。
-
多节段CSM的手术治疗通常可分为后路、前路或者前后路联合手术,但术式的选择方面客观标准存在差异,临床报道结果不一,尚存一定争议。前路手术支持者认为,前路手术减压能够直接将源于脊髓前方的压迫解除,改善颈椎生理曲度,有助于恢复、维持颈椎稳定性[5]。后路手术支持者认为,后路手术能够采用“脊髓飘移技术”对脊髓压迫进行间接减压,手术创伤小,最大程度上使颈椎活动度得以保留,邻近节段退变率较低。本研究对≥3个节段的脊髓受压的多节段CSM病人采用后路单开门椎管扩大成形术,近期手术优良率达到79.17%,与杨宝林等[6]报道结果一致,该术式操作简单、安全,效果肯定。但值得注意的是,无论是前路手术还是后路手术,对于多节段CSM进行单纯减压治疗时,即使由经验丰富的外科医师操作也仍有部分病人神经功能未能获得有效改善,因此探讨其疗效的自身影响因素对手术治疗的改进具有十分重要的意义。
本研究结果显示,病程>2年是多节段CSM椎管扩大成形术疗效的独立危险因素之一,与李泽龙等[7]的观点相一致,该研究发现CSM病程每增加6个月,获得理想疗效(JOA评分≥16)的概率降低接近22%。其原因在于,病程较长者脊髓传导束受压可能造成继发性脊髓缺血、脱髓鞘改变等,长期压迫可能导致不可逆的脊髓病理、生理改变,受压解除后脊髓营养供应虽有所改善,但变性部分脊髓神经功能很难再生,因此病程长的病人术后恢复差[8]。术前JOA评分是评估病人术前神经功能的重要指标,术前JOA评分越低说明CSM症状越严重,提示脊髓受压程度较重,该类病人术后预后不佳的机制与病程大致相似,主要源于其可能已经发生了不可逆的脊髓病理、生理改变,单纯的手术减压后很难获得较为优良的神经功能改善效果[9]。因此在明确诊断为CSM后,尤其是多节段受累者,应采取积极讨论治疗方案尽早进行治疗,并避免剧烈活动、负重以及外伤。
致压物最大径>5 mm、脊髓漂移距离 < 2.6 mm、平均压迫率>30%是影响多节段CSM手术治疗疗效的三项影像学因素,其均与脊髓压迫程度、解除压迫效果有关[10]。致压物最大径较大时即表明椎体后缘骨刺、突出椎间盘体积较大,最大径受压部位通常出现MRI T2加权像的高信号,脊髓可能发生炎症、水肿、缺血、脊髓软化、神经胶质增生等,脊髓功能受损通常更加严重,同时术中减压时对脊髓的冲击程度越大,进而影响预后。平均压迫率>30%与致压物最大径对手术疗效的影响机制大致相似[11]。柳万国等[12]通过最大致压物直径ROC曲线的绘制后得到最大直径4.95 mm以及平均压迫率30%为术后优良与非优良的预测临界值,本研究结果与之相符。有效的脊髓漂移距离在CSM后路减压手术的疗效预测中一直被反复探讨,脊髓漂移距离不仅与手术减压效果有关,同时也受到病人自身椎体后缘骨刺、椎间盘突出、钩椎关节增生程度的影响[13]。单纯后路手术对于靠近前方压迫的间接减压是以脊髓后移为基础的,然而脊髓漂移距离较短时可能会导致脊髓的后移无法完全脱离椎管靠前方的致压物,进而影响后路手术脊髓功能的恢复,降低神经功能改善率[14]。
综上所述,椎管扩大成形术是治疗多节段CSM的有效方法,近期疗效受到病程较长、脊髓压迫程度高、术前神经功能差等自身因素的影响。
多节段脊髓型颈椎病椎管扩大成形术疗效的自身影响因素研究
Study on the self-influencing factors of the therapeutic effecs of expansive laminoplasty for multilevel cervical spondylotic myelopathy
-
摘要:
目的探讨多节段脊髓型颈椎病(CSM)后路单开门椎管扩大成形术疗效的自身影响因素。 方法选择2016年12月至2018年12月120例多节段CSM病人为研究对象,均采用椎管扩大成形术治疗,随访1~3年,末次随访采用日本骨科协会(JOA)评分评价临床疗效,并设为由优良组与可差组。收集病人性别、年龄、病程等一般资料,计算致压物最大径、平均压迫率等影像学参数,组间通过单因素及多因素分析调查影响疗效的独立影响因素。 结果120例病人末次随访疗效评价优34例,良61例,可20例,差5例,优良率79.17%;优良组与可差组病程、年龄、致压物最大径、平均压迫率、脊髓漂移距离、术前Cobb角、术前JOA评分差异均具有统计学意义(P < 0.05~P < 0.01);2组性别、患病节段数差异均无统计学意义(P>0.05);多因素logistic回归分析显示,病程>2年、致压物最大径>5 mm、脊髓漂移距离 < 2.6 mm、平均压迫率>30%、术前JOA评分 < 10分是影响多节段CSM椎管扩大成形术疗效的独立危险因素(P < 0.05)。 结论椎管扩大成形术是治疗多节段CSM的有效方法,临床疗效受到病程较长、脊髓压迫程度高、术前神经功能差等自身因素的影响。 Abstract:ObjectiveTo explore the self-influencing factors of curative effects of posterior cervical expansive single open-door laminoplasty multlevel cervical spondylotic myelopathy(CSM). MethodsA total of 120 patients with multlevel CSM from December 2016 to December 2018 were treated with expansive laminoplasty, and followed up for 1 to 3 years.At the last follow-up, the patients were divided into the excellent group and poor group according to the the clinical efficacy evaluated by Japanese Orthopaedic Association(JOA) score.The general data such as gender, age and disease course of patients were collected, and the maximum diameter and average compression rate of pressure objects of the image data were calculated.The independent influencing factors of the curative effects between groups were investigated using the single factor and multi-factor analysis. ResultsAmong 120 patients, the results of the last follow-up showed that the excellent in 34 cases, good in 61 cases, fair in 20 cases and poor in 5 cases were found, and the excellent and good rate of which was 79.17%.The differences of the disease course, age, maximum compression diameter, mean compression rate, spinal drift distance, preoperative Cobb angle and preoperative JOA score between two groups were statistically significant(P < 0.05 to P < 0.01).The differences of the sex and number of disease segments between two groups were not statistcially significant(P>0.05).The results of multivariate logistic regression analysis showed that the course of disease more than 2 years, maximum diameter of the pressure object more than 5 mm, spinal cord drift distance less than 2.6 mm, average compression rate more than 30% and preoperative JOA score less than 10 were the independent risk factor affecting the efficacy of expansive laminoplasty for multlevel CSM. ConclusionsThe spinal enlargement is an effective method for treating multilevel CSM.The clinical efficacy is affected by its own factors such as longer course of disease, high degree of spinal cord compression and poor neurological function before surgery. -
表 1 多节段CSM椎管扩大成形术疗效单因素分析
因素 优良组(n=95) 可差组(n=25) χ2 P 病程/年 < 1 59 7 1~2 25 10 5.83 < 0.05 > 2 11 8 年龄/岁 ≤60 74 13 6.66 < 0.05 > 60 21 12 术前JOA评分/分 < 10 20 11 4.75 < 0.05 ≥10 75 14 性别 男 54 15 0.08 > 0.05 女 41 10 患病节段数 三节段 71 17 0.46 > 0.05 四节段 24 8 致压物最大径/mm > 5 80 15 7.03 < 0.05 ≤5 15 10 平均压迫率/% > 30 70 13 4.36 < 0.05 ≤30 25 12 脊髓漂移距离/mm < 2.6 15 9 5.05 < 0.05 ≥2.6 80 16 术前Cobb角/(°) > 10 65 11 5.08 < 0.05 ≤10 30 14  下载: 导出CSV
下载: 导出CSV
表 2 多节段CSM椎管扩大成形术疗效多因素分析
影响因素 B SE Waldχ2 P OR(95%CI) 病程>2年 0.911 0.306 8.89 < 0.05 2.487(1.431~7.786) 致压物最大径>5 mm 1.135 0.310 13.41 < 0.05 3.112(1.265~12.271) 脊髓漂移距离 < 2.6 mm 0.913 0.307 8.88 < 0.05 2.439(1.176~7.471) 平均压迫率>30% 1.107 0.324 11.68 < 0.05 3.026(1.519~8.080) 术前JOA评分 < 10分 1.047 0.321 10.65 < 0.05 2.855(1.640~11.232)
下载: 导出CSV
-
[1] 唐少龙, 黄庆华, 蒋会平, 等. 一期颈椎改良后路联合前路减压治疗不稳定型多节段脊髓型颈椎病[J]. 临床骨科杂志, 2017, 20(2): 129. doi: 10.3969/j.issn.1008-0287.2017.02.001 [2] 张华庆, 申才良, 张建湘, 等. 术前MRI测量脊髓受压程度与脊髓型颈椎病手术疗效的相关性研究[J]. 颈腰痛杂志, 2018, 36(6): 774. [3] TANG BS, YAN C, ZHANG XK, et al. Comparative analysis of two hybrid technique in treating multilevel cervical spondylotic myelopathy via anterior approach[J]. China J Orthop Traumatol, 2018, 31(11): 1034. [4] 康猛, 宋振全, 潘冬生, 等. 影响颈椎后路减压内固定术治疗脊髓型颈椎病预后的影像学因素分析[J]. 中国脊柱脊髓杂志, 2019, 29(9): 799. doi: 10.3969/j.issn.1004-406X.2019.09.04 [5] 关晓明, 马迅. 脊髓型颈椎病手术入路及减压融合方式的选择策略[J]. 中华骨科杂志, 2019, 39(23): 1478. doi: 10.3760/cma.j.issn.0253-2352.2019.23.009 [6] 杨宝林, 张绍东, 王小虎, 等. 颈椎后路改良单开门椎管扩大成形术治疗多节段脊髓型颈椎病的疗效分析[J]. 中国脊柱脊髓杂志, 2018, 28(4): 8. [7] 李泽龙, 廖文胜, 朱忠培. 颈后路单开门椎管扩大成形术治疗脊髓型颈椎病的影响因素[J]. 河南医学研究, 2017, 26(5): 798. doi: 10.3969/j.issn.1004-437X.2017.05.014 [8] 唐勇, 贾治伟, 吴剑宏, 等. 脊髓型颈椎病预后相关因素的研究进展[J]. 中国骨伤, 2016, 29(3): 216. doi: 10.3969/j.issn.1003-0034.2016.03.005 [9] 蔡奇霖, 张智, 郑佳状. 后路单开门椎管扩大成形术与前路植骨融合内固定术治疗多节段脊髓型颈椎病的疗效比较[J]. 临床和实验医学杂志, 2018, 17(10): 1074. doi: 10.3969/j.issn.1671-4695.2018.10.022 [10] 梁硕, 关海山. 多节段脊髓型颈椎病髓内MRI T2WI高信号强度比值分级与预后相关性分析[J]. 实用骨科杂志, 2019, 25(7): 588. [11] 关晓明, 马迅. 脊髓型颈椎病手术入路及减压融合方式的选择策略[J]. 中华骨科杂志, 2019, 39(23): 1478. doi: 10.3760/cma.j.issn.0253-2352.2019.23.009 [12] 柳万国, 庄新明, 许进. DTI在脊髓型颈椎病诊断及预后判定中应用的研究进展[J]. 中国骨与关节损伤杂志, 2017, 32(11): 1230. doi: 10.7531/j.issn.1672-9935.2017.11.049 [13] 李翔, 陆瓞骥, 胡勇. 磁共振弥散张量成像对脊髓型颈椎病病人术后神经功能恢复的预测作用[J]. 中国脊柱脊髓杂志, 2019, 29(5): 385. doi: 10.3969/j.issn.1004-406X.2019.05.01 [14] 王涛, 尚平福, 徐钦华, 等. 限制性椎板减压联合侧块螺钉固定对脊髓性颈椎病病人术后神经功能及轴性症状的影响[J]. 中国医学装备, 2019, 16(8): 70. -

 点击查看大图
点击查看大图
图(4)表(2)
计量
- 文章访问数: 1597
- HTML全文浏览量: 847
- PDF下载量: 2
- 被引次数: 0
